If your running shoes wear out quickly on the inner side or you often feel pain in your feet, knees, or lower back after walking, overpronation could be the underlying cause. Overpronation is a common biomechanical issue where the foot rolls excessively inward during the gait cycle—far beyond the normal range needed for shock absorption. While some inward motion (pronation) is natural and essential, excessive pronation disrupts how your body transfers weight and absorbs impact, leading to inefficient movement and increased injury risk.
This condition doesn’t just affect your feet—it triggers a chain reaction known as the kinetic chain effect, altering joint alignment from your arches all the way up to your spine. Left unaddressed, overpronation can contribute to plantar fasciitis, shin splints, knee pain, and chronic low back discomfort. The good news? With the right footwear, targeted exercises, and gait adjustments, you can correct the imbalance and restore smooth, pain-free movement. In this guide, you’ll learn how overpronation develops, how it impacts your entire body, and science-backed strategies to manage it effectively.
How Overpronation Disrupts Normal Foot Function
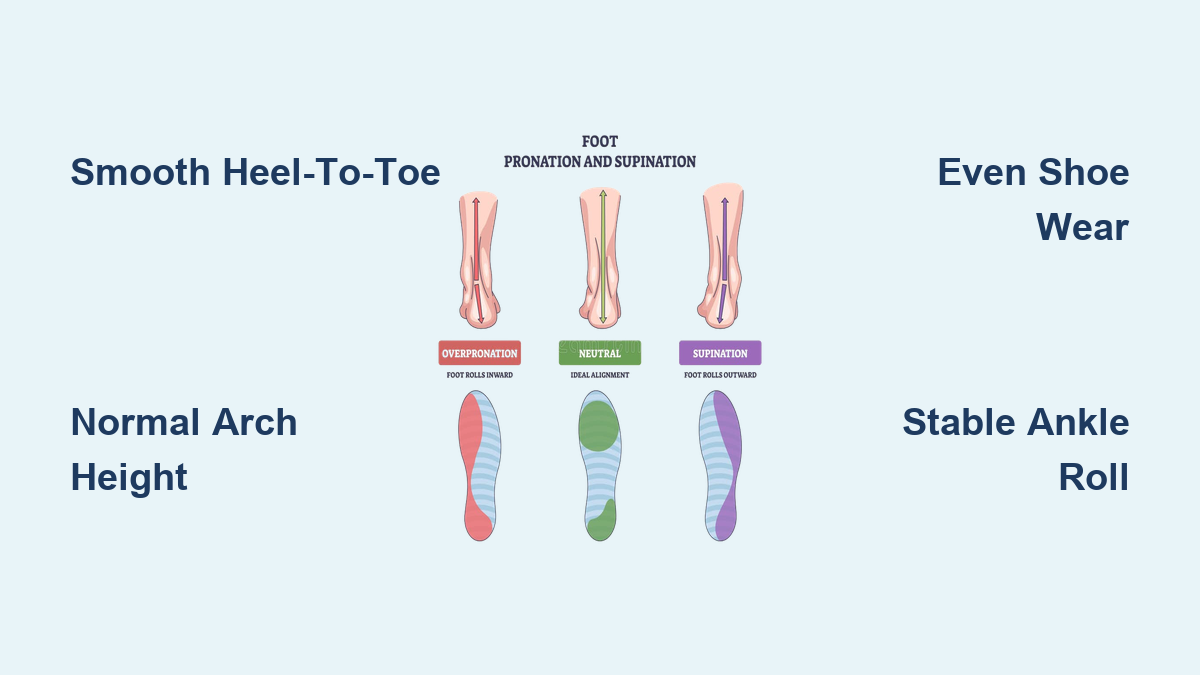
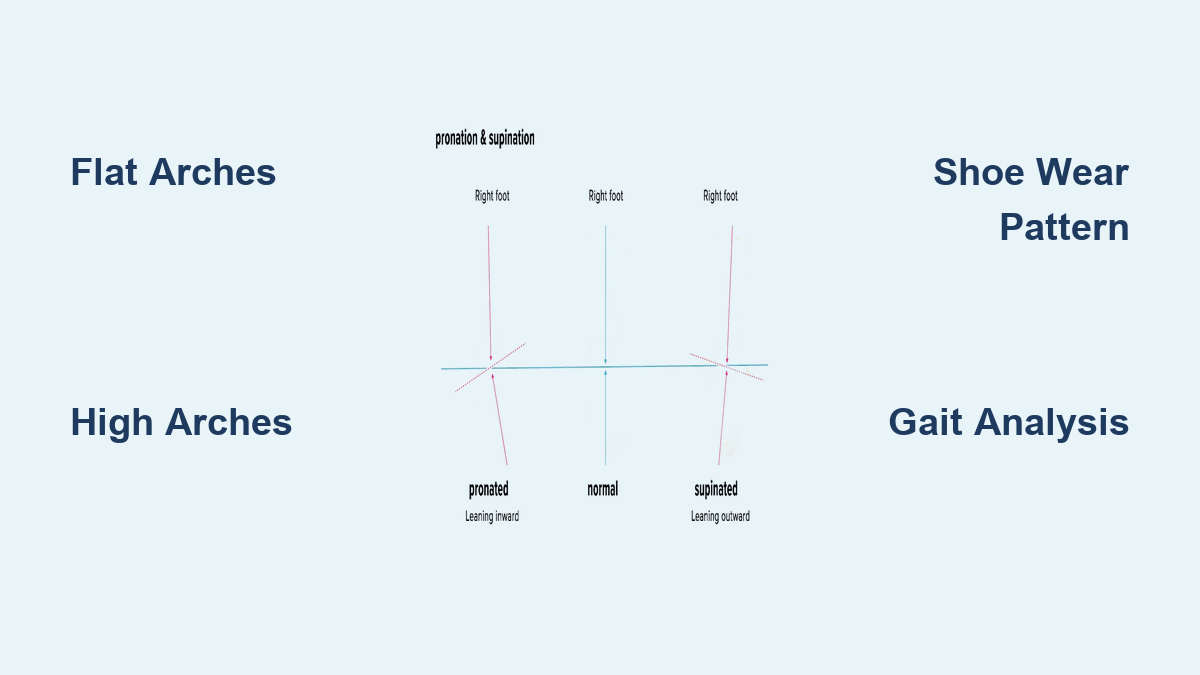
Normal Pronation vs. Excessive Inward Roll
Pronation is a natural foot motion that helps your foot adapt to the ground and cushion impact. When your heel strikes, the foot rolls inward about 15%, allowing the arch to flatten slightly and absorb force. This flexibility enables the foot to conform to uneven surfaces and prepare for push-off.
Overpronation occurs when this inward roll exceeds functional limits. Instead of stabilizing by midstance, the foot continues collapsing inward—often flattening the arch completely. This excessive medial roll prevents the foot from transitioning into a rigid lever during propulsion, reducing walking and running efficiency. The push-off becomes unstable, forcing other muscles and joints to compensate and increasing strain on soft tissues.
Delayed Supination and Weak Push-Off
In healthy gait, the foot shifts from pronation to supination—a stiffening process that locks the midfoot bones together for strong, efficient toe-off. With overpronation, this transition is delayed or incomplete. The foot remains too flexible when it should be rigid, causing energy loss and diminished forward drive.
As a result, propulsion relies more heavily on the big toe and second toe, increasing stress on the medial forefoot. This inefficient push-off contributes to fatigue, reduced performance, and long-term strain on key stabilizers like the posterior tibialis tendon.
What Causes Excessive Foot Rolling?
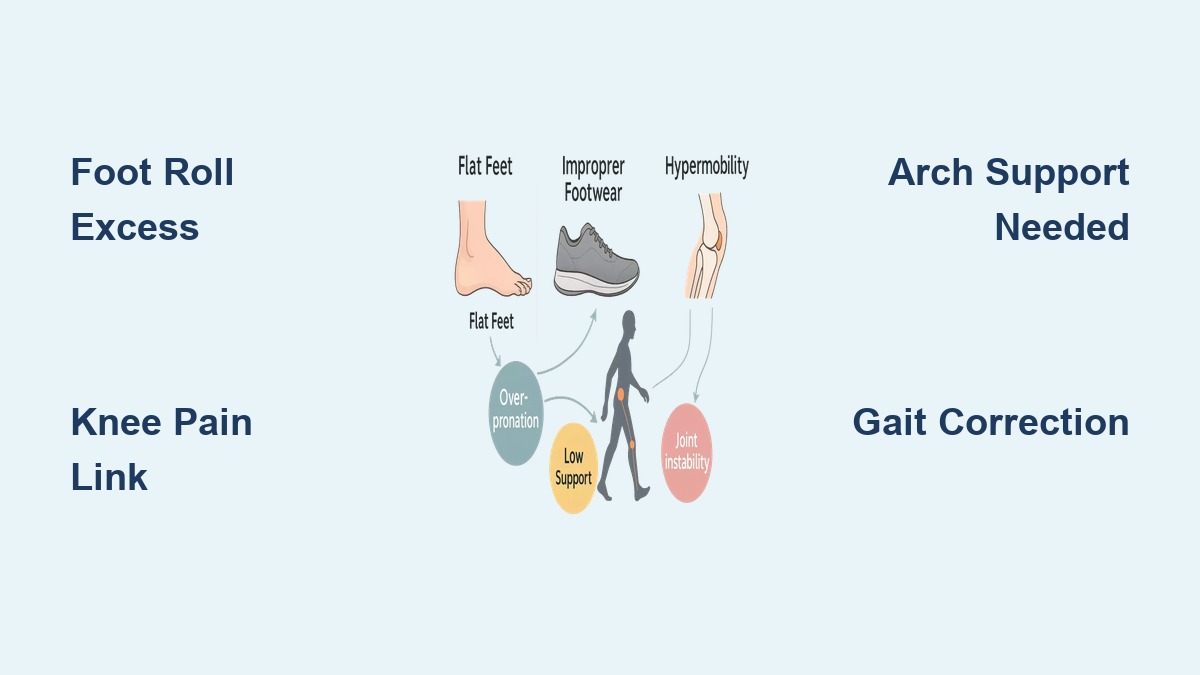
Structural and Genetic Factors
Some people are genetically predisposed to overpronation. Flat feet (pes planus)—where the medial arch is low or absent—are a primary structural cause. This may be present from birth or develop over time due to weak arch support.
Other inherited traits include ligament laxity, which allows joints to move beyond their normal range, and congenital foot deformities like tarsal coalition. A family history of flat feet or hypermobility increases your likelihood of developing overpronation, even if symptoms don’t appear immediately.
Functional and Lifestyle Triggers
Even with normal foot structure, daily habits can lead to acquired overpronation:
- Weak stabilizing muscles: Underactive posterior tibialis, gluteus medius, and intrinsic foot muscles fail to control arch collapse
- Tight calf and hip muscles: Restricted gastrocnemius, soleus, hamstrings, and TFL pull the leg into positions that encourage inward foot roll
- Excess body weight: Increased load on the arches accelerates flattening over time
- Poor footwear: Shoes without arch support or motion control allow unchecked pronation
- Prolonged standing or hard surfaces: Repetitive stress without recovery weakens foot integrity
The good news? These modifiable factors mean overpronation isn’t always permanent—it can often be corrected with targeted interventions.
How to Spot Overpronation: Telltale Signs
Visual Clues in Shoes and Stance
One of the easiest ways to identify overpronation is by checking your shoes. Look for excessive wear on the inner side of the heel and forefoot. If the sole is noticeably thinned along the medial edge, your foot is rolling too far inward with each step.
When standing barefoot, observe your arches. Do they appear flattened or collapsed? In severe cases, the entire sole touches the floor. You may also notice your feet pointing outward more than usual—a compensatory move to stabilize the unstable arch.
Try the wet footprint test: Wet your feet and step onto a surface that shows the print. A broad connection between heel and forefoot (more than half the width) indicates overpronation.
Common Pain Patterns Linked to Overpronation
Overpronation often leads to recurring discomfort:
- Arch or heel pain, especially in the morning (sign of plantar fasciitis)
- Shin tenderness along the inner leg (shin splints)
- Knee pain, particularly behind or around the kneecap
- Hip or low back aches after prolonged activity
- Ankle instability, with frequent “giving way” sensations
These symptoms may develop gradually as joint misalignment and muscle imbalances worsen over time.
The Full-Body Impact: How Overpronation Affects the Kinetic Chain
From Foot to Knee: The Domino Effect
Overpronation doesn’t stop at the foot—it sends ripple effects up the body. As the heel tilts inward (rearfoot eversion), it forces the shin bone (tibia) to rotate internally. This misalignment pulls the knee inward, creating a valgus (knock-kneed) position.
This abnormal knee tracking increases pressure on the patellofemoral joint, raising the risk of runner’s knee and IT band syndrome. The greater the foot collapse, the more the knee must compensate, especially during running or jumping.
Hip and Pelvic Misalignment
Internal tibial rotation continues upward, affecting the femur and hip. The gluteus medius and maximus—key stabilizers—become inhibited, reducing their ability to control pelvic drop during single-leg stance.
Over time, this can cause hip pain, trochanteric bursitis, and pelvic tilt. Bilateral overpronation often leads to anterior pelvic tilt, increasing lumbar curvature (lordosis) and contributing to lower back pain.
Spinal Stress and Postural Changes
Altered pelvic alignment disrupts spinal curves. Increased lordosis places extra strain on the lower back, while sacroiliac (SI) joints experience uneven shear forces. These changes may lead to chronic low back pain and reduced core stability, especially during dynamic activities.
Collectively, these issues form a pattern known as Pronation Distortion Syndrome, a postural dysfunction linked to poor gait mechanics and recurring injuries.
Injuries Associated with Overpronation
Foot and Ankle Conditions
Overpronation places abnormal stress on soft tissues and joints:
- Plantar fasciitis: Excessive arch strain inflames the plantar fascia
- Posterior tibial tendon dysfunction (PTTD): The tendon that supports the arch becomes overworked and weakens
- Achilles tendinitis: Altered heel position increases tension on the Achilles
- Bunions (hallux valgus): Misdirected forces push the big toe inward
- Morton’s neuroma: Nerve compression between metatarsals due to poor weight distribution
These conditions often start subtly but worsen without intervention.
Lower Limb and Joint Injuries
The chain reaction extends beyond the foot:
- Shin splints (medial tibial stress syndrome): Overuse of the tibialis posterior muscle
- Stress fractures: Repetitive overload in the tibia, navicular, or metatarsals
- IT band syndrome: Friction from altered knee mechanics
- Patellofemoral pain syndrome: Pain from kneecap misalignment
- Hip bursitis: Inflammation due to poor gluteal function and pelvic instability
Athletes and active individuals are especially vulnerable during high-impact activities.
How to Diagnose Overpronation Accurately

Clinical Gait and Posture Assessment
The most accurate diagnosis comes from a podiatrist, physical therapist, or sports medicine specialist. They use:
- Treadmill gait analysis: Observing foot strike, arch collapse, and limb alignment
- Video motion capture: Slow-motion review of joint angles and timing
- Overhead squat test: Checking for foot flattening, knee valgus, and pelvic tilt
These assessments reveal functional deficits not visible in static stance.
Key Diagnostic Tests
- Navicular drop test: Measures how much the navicular bone drops when standing. A drop greater than 10 mm indicates significant overpronation.
- Pressure mapping: Uses in-shoe or platform sensors to show center of pressure (COP) trajectory and plantar load distribution.
- Wet footprint test: A simple at-home method—broad midfoot contact suggests overpronation.
For complex cases, X-rays or MRI may be used to rule out structural deformities or tendon damage.
Proven Management Strategies for Overpronation
Choose Supportive Footwear That Corrects Motion

Footwear is the first line of defense. Look for:
- Motion-control or stability shoes: Designed to limit excessive inward roll
- Medial post or dual-density midsole: Denser foam on the inner side resists collapse
- Firm heel counter: Stabilizes the rearfoot and reduces eversion
- Arch support: Built-in structure to support the medial longitudinal arch
- Straight or semi-curved last: Offers more stability than curved lasts
Stability shoes suit mild to moderate overpronation; motion-control shoes are better for severe cases or flat feet.
Use Orthotics to Improve Alignment
Both custom and over-the-counter (OTC) insoles can correct foot mechanics.
- Custom orthotics: Made from a foot mold, prescribed by a podiatrist for precise correction
- OTC insoles: Affordable options like Dr. Scholl’s® Stabilizing Support Insoles offer:
- Arch support
- Medial posting
- Shock-absorbing heel cup
- Motion control shell
Orthotics help realign the subtalar joint, reduce rearfoot eversion, and decrease strain on tendons and ligaments.
Retrain Your Gait with Science-Backed Techniques
Effective Gait Modifications
Gait retraining is a low-cost, effective way to reduce overpronation.
Modify Foot Progression Angle
Turning your feet slightly inward (toe-in gait) by 5°–10° reduces rearfoot eversion. A 2023 meta-analysis found this change reduces peak eversion by 2.1° on average.
How to do it: Practice walking with toes pointing straight ahead or slightly inward. Use mirrors or video feedback to monitor form.
Shift Center of Pressure Laterally
Consciously shifting weight toward the outer edge of the foot reduces pronation. Studies show a -3.3° reduction in rearfoot eversion with COP lateralization.
Tip: Imagine balancing over the “tripod” of your foot—heel, big toe, and little toe—while favoring the outer side during stance.
Adopt a Forefoot or Midfoot Strike
Heel striking amplifies impact and encourages overpronation. Landing on the midfoot or forefoot increases arch stiffness and reduces braking forces.
Caution: Transition gradually to avoid calf strain.
Increase Step Rate
Raising your cadence by 5–10% shortens your stride, reduces foot inclination, and decreases pronation.
Try it: Use a metronome app to match steps per minute (e.g., from 160 to 176 spm).
Adjust Step Width
While research shows no significant effect on rearfoot eversion overall, some individuals benefit from wider steps, which may improve pelvic stability.
Avoid excessively narrow steps, which can increase inward collapse.
Strengthen Weak Muscles, Stretch Tight Ones
Targeted Strengthening Exercises
Correcting muscle imbalances is key to long-term improvement.
Focus on These Muscles:
- Posterior tibialis: Single-leg heel raises with inward rotation
- Anterior tibialis: Resisted dorsiflexion with a band
- Gluteus medius: Clamshells, side-lying leg lifts
- Gluteus maximus: Glute bridges, single-leg deadlifts
- Intrinsic foot muscles: Towel scrunches, marble pickups, short foot exercise
Perform 2–3 sets of 10–15 reps, 3–4 times per week.
Follow the NASM Corrective Exercise Continuum
- Inhibit: Foam roll overactive muscles (calves, peroneals, IT band, hamstrings)
- Lengthen: Stretch tight areas (calf, TFL, hip flexors)
- Activate: Isolate weak muscles (e.g., short foot drill)
- Integrate: Combine into functional moves (e.g., single-leg squat with alignment control)
This phased approach ensures lasting neuromuscular changes.
Essential Stretching Routine
Tight muscles pull the body out of alignment. Stretch daily:
– Calf stretch (gastrocnemius and soleus): Hold 30 seconds per leg
– Plantar fascia stretch: Pull toes toward shin while seated
– Hamstring stretch: Keeps pelvis neutral
– TFL and IT band stretch: Reduces lateral tension affecting the knee
Final Note: Overpronation is more than a foot issue—it’s a full-body biomechanical challenge. By understanding its causes and effects, you can take control with proper footwear, targeted exercises, and gait adjustments. Early intervention prevents long-term damage and keeps you moving efficiently, comfortably, and pain-free. Whether you’re a walker, runner, or on your feet all day, addressing overpronation is a smart investment in your mobility and musculoskeletal health.