If you live with diabetes, a tiny cut on your foot might not hurt—but it could be the start of something far more serious. Due to nerve damage and poor circulation, even minor injuries can go unnoticed and fail to heal, leading to infections, ulcers, and in severe cases, amputation. This is why special foot care products aren’t just a convenience—they’re a medical necessity for people with diabetes.
Diabetic peripheral neuropathy affects up to 50% of individuals with Type 2 diabetes, dulling sensation in the feet and making injuries easy to miss. Combine this with reduced blood flow from peripheral vascular disease, and the body loses its ability to fight infection or repair tissue. As a result, 1 in 12 people with diabetes will develop a foot ulcer, and these ulcers are the leading cause of non-traumatic lower-limb amputations in this population. But here’s the hopeful truth: up to 85% of amputations can be prevented with proper daily care and the right tools.
Standard socks, shoes, and skincare products simply aren’t designed for these unique risks. They can restrict circulation, create friction, or fail to protect vulnerable skin. That’s where diabetic-specific foot care products come in—engineered to prevent injury, support healing, and compensate for loss of sensation. From seamless socks to custom orthotics and smart monitoring tools, each product plays a critical role in protecting foot health.
In this guide, you’ll learn exactly how diabetes affects the feet, why regular products fall short, and how specialized tools help prevent complications. You’ll also discover a proven daily foot care routine, warning signs that demand immediate attention, and how working with a healthcare team can protect your mobility—and your life.
Diabetic Neuropathy: Why You Can’t Feel Injuries
Loss of Protective Sensation
High blood sugar over time damages nerves in the hands and feet, a condition known as diabetic peripheral neuropathy. This nerve damage reduces or completely eliminates the ability to feel pain, heat, or pressure in the feet. Without this protective sensation, you might step on a sharp object, develop a blister from tight shoes, or even burn your foot in hot bathwater—and not realize it.
Because pain is the body’s alarm system, losing it means injuries can go undetected for days or weeks. A small blister can turn into a deep ulcer, especially when combined with poor circulation. Shockingly, nearly half of all patients with neuropathy have no symptoms, making daily visual inspection essential.
Early Signs of Nerve Damage
While some people feel no pain, others experience early warning signs:
– Tingling or “pins and needles” in the feet
– Burning pain, often worse at night
– Numbness that starts in the toes and moves upward
– Muscle weakness or balance issues
– Dry, cracked skin due to impaired sweat gland function
If you notice any of these symptoms, speak with your doctor. A simple monofilament test or tuning fork exam can detect nerve damage early—before serious complications arise.
Poor Circulation: Why Wounds Won’t Heal
Blocked Blood Flow to Feet
Diabetes accelerates atherosclerosis, the narrowing and hardening of arteries, which reduces blood flow to the lower limbs—a condition called peripheral vascular disease (PVD). With less blood reaching the feet, oxygen, nutrients, and infection-fighting white blood cells can’t get to injured tissue efficiently.
Even a small cut may take weeks to heal—or never close at all. Without adequate circulation, antibiotics struggle to work, and tissue death (gangrene) becomes a real risk. This is especially dangerous when combined with neuropathy, as the patient may not feel the worsening injury.
Warning Signs of Poor Blood Flow
Look for these red flags:
– Feet that feel cold or appear pale, blue, or dusky
– Leg pain when walking (claudication)
– Slow-growing, thick toenails
– Hair loss on legs or feet
– Weak or absent pulses in the feet
A healthcare provider can assess circulation using a Doppler ultrasound or ankle-brachial index (ABI) test. If blood flow is severely limited, a vascular specialist may be needed to restore it.
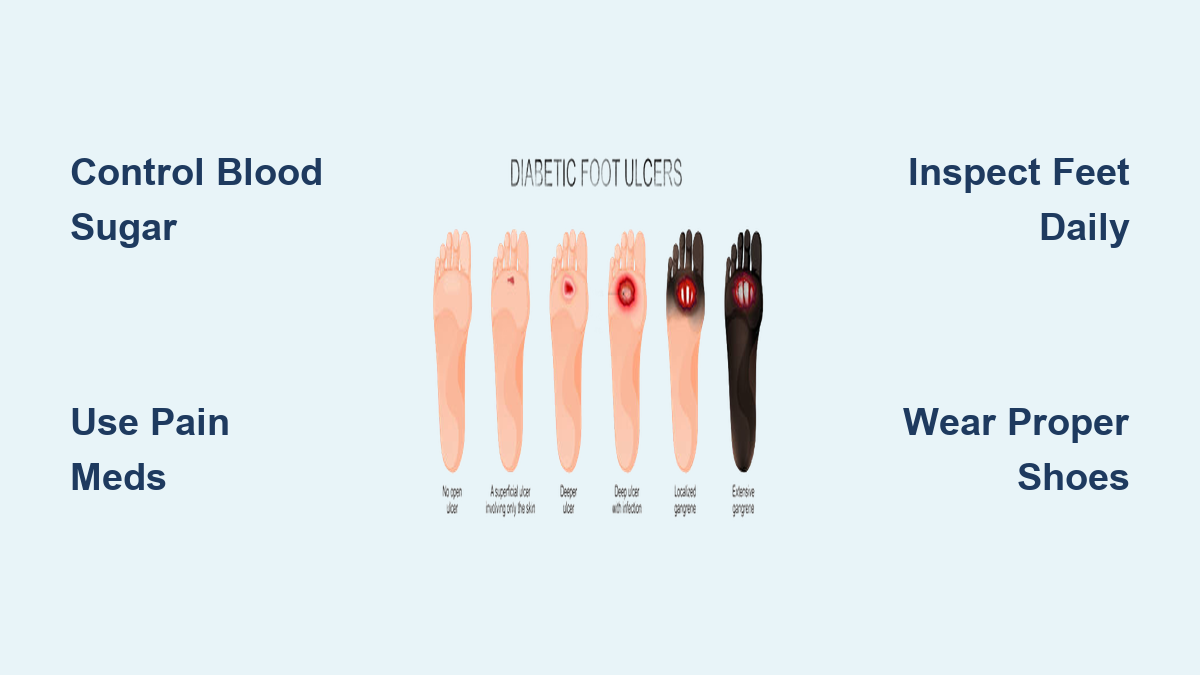
Diabetic Foot Ulcers: How They Start and Spread

The Silent Progression
When neuropathy and poor circulation combine, the risk of diabetic foot ulcers (DFUs) skyrockets. These open sores usually form on high-pressure areas like the ball of the foot, heel, or under the toes. Because the patient can’t feel discomfort, friction from ill-fitting shoes or walking barefoot can create calluses that break down into ulcers.
Once an ulcer forms, infection can spread rapidly through compromised tissue. Without prompt treatment, it can reach deep into muscles, tendons, or even bone.
Consequences of Untreated Ulcers
Left untreated, DFUs can lead to:
– Cellulitis (skin infection)
– Abscesses
– Osteomyelitis (bone infection)
– Gangrene
– Amputation
In the U.S., over 170,000 lower-limb amputations occur annually in adults with diabetes—most starting from a preventable foot ulcer.
Why Regular Foot Products Aren’t Enough
Risks of Standard Socks and Shoes
Everyday footwear and footcare items are made for healthy feet, not for diabetic vulnerabilities.
- Regular socks often have tight elastic tops that cut off circulation and internal seams that rub against numb skin, causing blisters.
- Off-the-shelf shoes may press on bony areas, create pressure points, or lack cushioning, increasing ulcer risk.
- Fragranced moisturizers can irritate sensitive skin.
- Toenail clippers used improperly can lead to cuts or ingrown nails.
Using non-specialized products is like driving without seatbelts—possible, but dangerously unnecessary.
Diabetic Socks: More Than Just Comfort
Seamless, Non-Binding Protection
Diabetic socks are medical-grade garments designed to prevent injury and support circulation.
Key features include:
– Seamless toes: Eliminate friction and blister risk
– Non-binding tops: No tight bands that restrict blood flow
– Moisture-wicking fabric: Keeps feet dry and reduces fungal infections
– Extra cushioning: Absorbs shock in high-pressure areas
– White interior (in some): Helps spot drainage from hidden wounds
Some advanced models, called smart diabetic socks, include sensors that track foot temperature. A rise in heat can signal inflammation before visible signs appear—giving users time to rest and seek care early.
When to Wear Them
Wear diabetic socks every day, even indoors. Change them if damp or soiled. Avoid socks with holes or stretched cuffs. Look for brands with the APMA Seal of Approval for added assurance.
Diabetic Shoes: Built to Prevent Ulcers

Designed for High-Risk Feet
Diabetic shoes are medical devices engineered to reduce pressure, prevent friction, and accommodate foot deformities like hammertoes or bunions.
Essential features:
– Extra depth and width: Fits swollen feet or custom orthotics
– Smooth interior lining: No seams or rough spots inside
– Rocker-bottom soles: Reduce pressure on the ball of the foot while walking
– Lightweight, breathable materials: Improve comfort
– Adjustable closures (Velcro): Easy to put on and customize fit
These shoes distribute weight evenly, minimizing shear forces that cause calluses and ulcers.
Getting Properly Fitted
Foot size changes over time—especially with diabetes. Always get your feet measured when buying shoes.
Fit tips:
– Shop in the afternoon, when feet are slightly swollen
– Wear the same sock type you’ll use daily
– Leave ½ inch between your longest toe and the shoe tip
– Shoes should be comfortable immediately—no “break-in” period needed
Ill-fitting shoes are a top cause of foot ulcers. Never wear shoes that pinch, slip, or feel tight.
Custom Orthotics: Redistribute Pressure Safely

Prescription Insoles That Protect
Over-the-counter insoles offer cushioning but not medical-grade support. Custom orthotics, prescribed by a podiatrist, are molded to your foot’s exact shape and correct biomechanical imbalances.
Benefits:
– Offload pressure from high-risk areas (e.g., metatarsal heads)
– Improve alignment and gait
– Prevent ulcers in patients with flat feet or high arches
– Support healing after an ulcer has formed
Used with diabetic shoes, orthotics form a powerful defense against recurring wounds.
Who Needs Them?
Recommended for patients with:
– History of foot ulcers
– Peripheral neuropathy
– Foot deformities
– Charcot foot
Medicare and many insurers cover therapeutic footwear and orthotics for qualifying diabetic patients—ask your provider.
Daily Foot Inspection: Catch Problems Early
Check Every Day—Even If You Feel Fine
Since you may not feel injuries, daily visual inspection is mandatory.
Use:
– Long-handled mirror to view soles
– Smartphone camera to photograph hard-to-see spots
– Monofilament test (clinical use) to check sensation
What to Look For
Inspect for:
– Cuts, blisters, redness, or swelling
– Bruises or discoloration (blue, black, pale)
– Calluses, corns, ingrown toenails
– Warm or hot spots (early inflammation)
– Fungal infections between toes
– Changes in foot shape
If you notice anything unusual, contact your healthcare provider the same day.
Skin and Nail Care: Avoid Hidden Dangers
Moisturize—But Not Between Toes
Dry, cracked skin creates entry points for infection. Apply fragrance-free, hypoallergenic lotion daily to the top and bottom of your feet.
⚠️ Never apply between toes—this area stays moist and prone to fungal growth. Instead, lightly dust with antifungal powder or cornstarch.
Safe Toenail Trimming
Trim toenails straight across—do not round the corners, which can lead to ingrown nails.
Steps:
1. Cut after bathing when nails are softer
2. Use clean, sharp clippers
3. File edges with an emery board
4. Never cut cuticles
If you have poor vision, thickened nails, or neuropathy, see a podiatrist for nail care. Never use acid-based products or razors on corns or calluses—they can cause burns.
Preventing Amputations: A Proven Strategy
The 30% Reduction from Team Care
A multidisciplinary approach slashes amputation rates. One study in Italy showed over a 30% drop in major amputations with coordinated care from endocrinologists, podiatrists, vascular surgeons, and wound care nurses.
Who’s at Highest Risk?
You need more frequent monitoring if you have:
– Neuropathy
– History of ulcers or amputation
– Peripheral vascular disease
– Foot deformities
– Poorly controlled blood sugar
High-risk patients should see a podiatrist every 3 to 6 months.
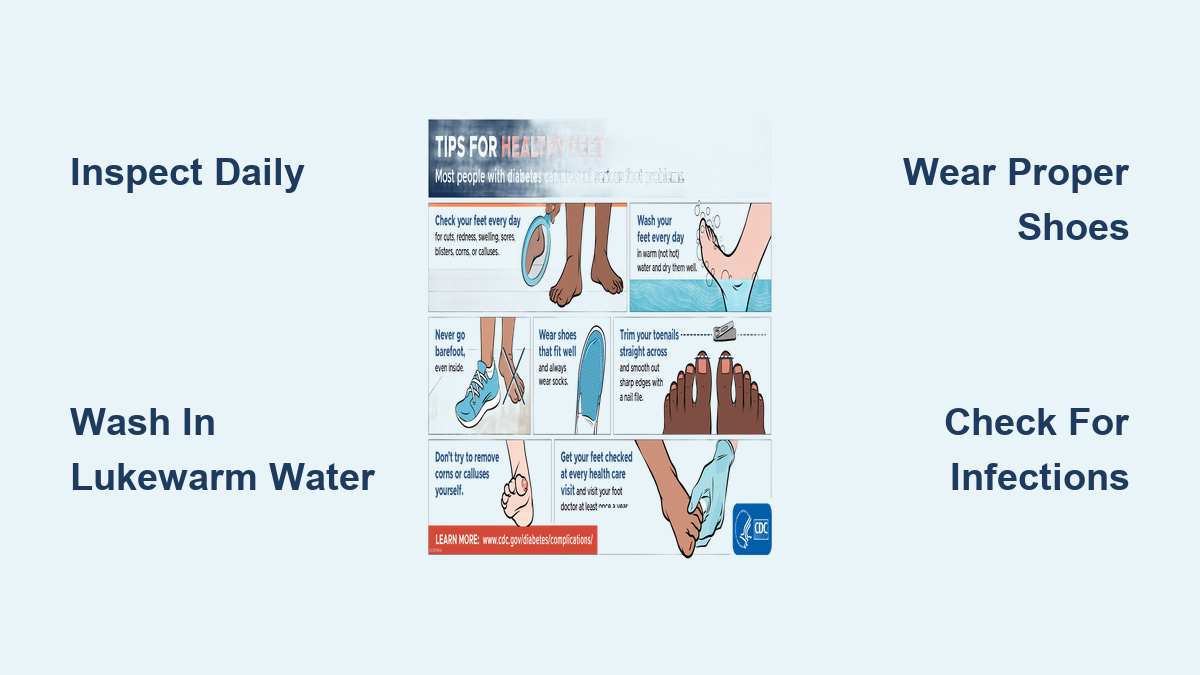
Daily Foot Care Routine: 8 Essential Steps
- Inspect feet daily using a mirror or phone
- Wash with lukewarm water—test with elbow, not feet
- Dry thoroughly, especially between toes
- Moisturize top and bottom—skip between toes
- Trim nails straight across, file edges
- Wear protective footwear—never barefoot
- Avoid temperature extremes—no heating pads or open sandals
- Control your ABCs: A1C <7%, BP <130/80, LDL <100, quit smoking
When to Seek Immediate Medical Help
Seek care immediately for:
– A cut or blister that doesn’t heal in a few days
– Redness, swelling, warmth, or pus
– Foul odor
– Black, blue, or pale skin
– New foot deformity
– Fever or chills with a foot wound
Early treatment saves limbs.
Final Note: Foot Health Is Lifesaving
For people with diabetes, foot care isn’t optional—it’s a daily act of self-preservation. The combination of numbness, poor blood flow, and slow healing makes every minor injury a potential crisis. But with the right tools and habits, most complications can be avoided.
Specialized products—diabetic socks, therapeutic shoes, orthotics, and inspection aids—are not luxuries. They are medical necessities that protect sensation, reduce pressure, prevent injury, and enable early detection.
Pair these tools with daily self-checks, professional foot exams, and tight blood sugar control, and you dramatically reduce your risk of ulcers and amputations. Your feet carry you through life—make their care a non-negotiable part of your routine.
Start today. Inspect your feet. Wear the right socks. See your podiatrist. Because prevention isn’t just possible—it’s in your hands.