You wake up with a tight, throbbing ache in your calf. It’s not quite like a muscle cramp—more like a deep, persistent pain that worsens when you walk. Your leg feels warm to the touch, looks slightly swollen, and maybe even has a reddish tint. You brush it off as overexertion or a minor strain. But what if it’s something far more serious?
Deep vein thrombosis (DVT) occurs when a blood clot forms in one of the deep veins—usually in the leg or foot—and can strike without warning. Alarmingly, up to half of all DVT cases show no symptoms until a life-threatening complication like pulmonary embolism (PE) occurs. Yet, when signs do appear, they often follow a distinct pattern that, if recognized early, can save lives. Each year, between 300,000 and 600,000 Americans develop blood clots in the leg or foot, and about 10–30% of those diagnosed die within one month—many due to undiagnosed or delayed treatment.
This guide breaks down the key signs of DVT in the leg and foot, explains why symptoms are often missed, and outlines when to seek emergency care. You’ll learn how to distinguish DVT from common mimics like muscle strains, understand risk factors, and recognize red flags for complications. With accurate, timely action, DVT is both treatable and preventable.
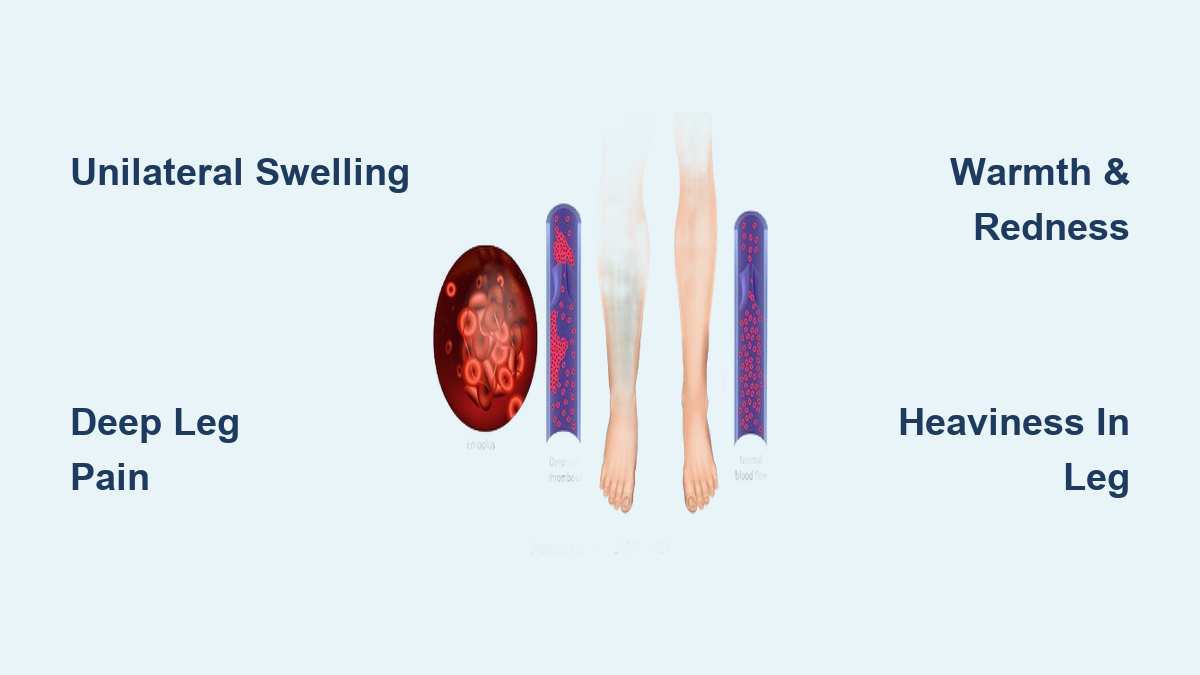
Unilateral Leg Swelling: A Major Warning Sign

Swelling in one leg is one of the most telling signs of DVT. Unlike general puffiness from standing too long or mild fluid retention, DVT-related swelling is unilateral—meaning it affects only one limb—and typically starts in the calf before spreading to the ankle, foot, or thigh.
Why Swelling Happens in DVT
The clot blocks normal blood flow back to the heart, causing blood and fluid to pool behind the obstruction. This results in visible enlargement and a tight, stretched feeling in the skin. The affected leg may measure over 3 cm larger in circumference than the other when measured at the same point (e.g., 10 cm below the tibial tuberosity).
What to Look For
- Sudden or gradual increase in leg size
- Pitting edema (skin retains an indentation when pressed)
- Swelling that doesn’t improve with elevation or rest
- Tightness in shoes or socks on one foot only
If your pants or socks fit noticeably tighter on one leg, don’t ignore it. This asymmetry is a critical clue.
DVT Leg Pain: Not Just a Cramp

Pain from DVT is often mistaken for a pulled muscle or “charley horse,” but there are key differences. The discomfort is deep, persistent, and progressive, originating in the calf or inner thigh along the path of the deep veins.
How DVT Pain Differs from Muscle Strain
| Feature | DVT Pain | Muscle Cramp/Strain |
|---|---|---|
| Onset | Gradual or sudden | Sudden, post-activity |
| Location | Deep, often calf or thigh | Superficial, specific muscle |
| Duration | Worsens over hours/days | Resolves in minutes/hours |
| Relief | No improvement with rest | Improves with stretching/rest |
| Aggravated by | Walking, standing, foot dorsiflexion | Movement of injured muscle |
Pain may intensify when walking or flexing the foot upward (dorsiflexion), a historical sign known as Homans’ sign—though this test is no longer relied upon due to inaccuracy.
Warmth and Redness Over the Clot Site

Inflammation around the clot triggers increased blood flow and heat production, making the skin over the affected area noticeably warmer than the opposite leg. This warmth is usually accompanied by redness or discoloration.
Skin Changes to Watch For
- Localized warmth when touching the calf or foot
- Red, flushed skin (in lighter skin tones)
- Darker, ashen, or purplish hue (in darker skin tones)
- Discoloration that may spread over time
Patients often detect warmth by comparing both legs with the back of their hands. If one side feels distinctly hotter, DVT should be suspected—even without severe pain.
Heaviness and Tightness in the Affected Leg
Many people with DVT describe a constant sense of heaviness or tightness, as if the leg is weighed down. This results from venous stasis and rising pressure in the limb.
Unlike normal fatigue after prolonged standing, this sensation:
– Persists despite rest
– Worsens by the end of the day
– Doesn’t resolve with sleep or leg elevation
– May interfere with walking or daily activities
This symptom is sometimes dismissed as aging or poor circulation, especially in older adults or those with varicose veins.
Visible Vein Changes and Numbness
While not always present, some individuals develop engorged superficial veins near the skin surface. These dilated veins form as collateral pathways try to bypass the blocked deep vein.
Additionally, reduced blood flow can cause nerve-related sensations, including:
– Numbness in the foot or lower leg
– Tingling or pins-and-needles
– Burning or itching under the skin
These neurological symptoms are often misdiagnosed as peripheral neuropathy—especially in diabetics—but their sudden, one-sided onset should raise suspicion for DVT.
Key Clues That It’s DVT—Not a Strain
DVT is frequently mistaken for benign conditions. But several features help differentiate it:
Unilateral Symptoms
DVT almost always affects one leg. Bilateral swelling or pain is more likely due to heart failure, kidney disease, or medication side effects.
No Recent Injury
Symptoms appear without trauma. If you didn’t twist your ankle or overwork your calf, a clot becomes more likely.
Progressive Worsening
Unlike minor strains that improve, DVT symptoms get worse over time—especially swelling and pain.
Combination of Signs
The presence of two or more symptoms—especially swelling, pain, warmth, and redness—greatly increases the likelihood of DVT.
When DVT Shows No Symptoms
Up to 50% of DVT cases are asymptomatic, making awareness of risk factors just as important as recognizing symptoms. Silent clots can still break loose and cause pulmonary embolism—the leading cause of preventable hospital death.
Even if you feel fine, consider DVT if you have:
– Recent surgery or hospitalization
– Prolonged immobility (long flight, bed rest)
– Active cancer or chemotherapy
– Use of estrogen-based medications
– Personal or family history of blood clots
In these cases, preventive measures like compression stockings or blood thinners may be recommended.
Risk Factors You Can’t Ignore
DVT arises from a mix of factors known as Virchow’s triad: slow blood flow, vessel damage, and increased clotting tendency. The more risk factors you have, the higher your chance of developing a clot.
High-Risk Medical Conditions
- Cancer: Releases procoagulant substances
- Heart failure: Slows circulation
- Obesity: Triples DVT risk; fivefold increase if severely obese
- Diabetes: Damages blood vessels
- Inflammatory diseases (e.g., IBD): Chronic inflammation raises clot risk
- Antiphospholipid syndrome or Factor V Leiden: Genetic or autoimmune clotting disorders
Lifestyle and Situational Triggers
- Long-haul travel (>4 hours): “Economy class syndrome”
- Surgery (especially hip/knee replacement): Immobility + tissue injury
- Fractures in leg/ankle: Damages veins and limits movement
- Smoking: Harms vessel walls and thickens blood
- Dehydration: Concentrates blood, slowing flow
Hormonal and Reproductive Risks
- Oral contraceptives or HRT: Estrogen increases clotting by 3–4x
- Pregnancy and postpartum (up to 12 weeks): Hormones + uterine pressure
- Recurrent miscarriages: May signal undiagnosed clotting disorder
Age and Family History
- Risk rises after age 40, sharply after 60
- Having a first-degree relative with DVT doubles your risk
- Genetic testing may be advised for unexplained clots
Pulmonary Embolism: The Life-Threatening Complication
The greatest danger of DVT is that the clot can break free and travel to the lungs, causing a pulmonary embolism (PE). This is a medical emergency—and can occur even if leg symptoms were mild or absent.
Warning Signs of PE
- Sudden shortness of breath
- Sharp chest pain that worsens with breathing
- Coughing up blood
- Rapid heartbeat
- Dizziness, fainting, or lightheadedness
- Excessive sweating
If you or someone else shows these signs, call 911 immediately. PE kills about 100,000 Americans annually—many within hours of symptom onset.
Post-Thrombotic Syndrome: A Chronic Aftermath
Even with treatment, up to 50% of DVT patients develop post-thrombotic syndrome (PTS)—a long-term condition caused by vein valve damage.
Symptoms include:
– Chronic leg swelling
– Aching or cramping
– Skin discoloration (brownish patches)
– Itching or dry, scaly skin
– Venous ulcers (open sores near the ankle)
PTS can severely impact mobility and quality of life. The best defense is early diagnosis and consistent use of compression stockings (30–40 mmHg), which reduce PTS risk by at least 50%.
How Doctors Diagnose DVT

You can’t confirm DVT on your own. Diagnosis requires clinical evaluation and testing.
Clinical Assessment
Your doctor will ask about:
– Symptom onset and progression
– Recent surgeries, travel, or immobility
– Medications (especially hormones)
– Personal and family history of clots
They’ll examine:
– Leg circumference (difference >3 cm is suspicious)
– Tenderness along deep veins
– Skin temperature and color
– Swelling and pitting edema
Confirmatory Tests
Duplex Ultrasound (First Choice)
- Gold standard for detecting clots in leg veins
- Uses sound waves to see blood flow and vein compressibility
- Non-invasive, fast, and highly accurate (~95% for clots above the knee)
D-Dimer Blood Test
- Measures a protein fragment released when clots dissolve
- Negative result in low-risk patients rules out DVT
- Positive result isn’t definitive—can be elevated in infection, pregnancy, or cancer
Advanced Imaging (if needed)
- CT Venography or CTPA: For suspected PE or pelvic clots
- MRI/MRV: Used in pregnancy or complex cases
- Venography: Rarely used; invasive with contrast dye
Treatment: Stopping Clots Before They Spread
The goal of DVT treatment is to prevent clot growth, stop PE, and reduce recurrence.
Anticoagulants (Blood Thinners)
These don’t dissolve clots but prevent new ones from forming. Most patients start on one of these:
Direct Oral Anticoagulants (DOACs) – Preferred
- Rivaroxaban (Xarelto)
- Apixaban (Eliquis)
- Dabigatran (Pradaxa)
- Edoxaban (Savaysa)
- No routine blood monitoring required
Other Options
- Low Molecular Weight Heparin (e.g., Lovenox): Injected daily; common in cancer patients and pregnancy
- Warfarin (Coumadin): Requires weekly INR checks; used if DOACs aren’t safe
- Unfractionated Heparin: IV use in hospitals
Treatment Duration:
– 3–6 months for provoked DVT (e.g., after surgery)
– Indefinite for unprovoked or recurrent clots
Compression Stockings
- Wear daily, starting at diagnosis
- Reduce swelling and lower PTS risk by 50%
- Use graduated 30–40 mmHg compression
Clot Removal (Severe Cases Only)
Reserved for massive clots threatening limb or life:
– Thrombolytic therapy (tPA): “Clot busters” via IV or catheter
– Mechanical thrombectomy: Device removes clot
– IVC filter: For patients who can’t take blood thinners
Prevent DVT Before It Starts
You can’t eliminate all risk, but you can dramatically reduce it.
Move Regularly
- Avoid sitting more than 2 hours at a time
- On long flights or drives: walk every 1–2 hours, do ankle circles and heel-toe raises
- At work: take stretch breaks every hour
Stay Hydrated and Healthy
- Drink water—dehydration thickens blood
- Maintain a healthy weight—obesity triples risk
- Quit smoking—it damages blood vessels
Medical Prevention
- Hospitalized or post-surgery patients: Ask about prophylactic anticoagulants or compression devices
- High-risk individuals: May need genetic screening for clotting disorders
When to Seek Emergency Care
Don’t wait. Seek immediate medical help if you have:
Signs of Pulmonary Embolism:
- Sudden shortness of breath
- Chest pain when breathing
- Coughing up blood
- Rapid heartbeat
- Fainting or dizziness
Severe DVT Warning:
- Sudden, severe leg swelling
- Pain and discoloration (blue or pale skin)
- Cold, numb leg—could indicate phlegmasia cerulea dolens, a limb-threatening emergency
For suspected DVT—unilateral swelling, pain, warmth, redness—contact your doctor the same day. Early treatment prevents catastrophe.
Final Note: Deep vein thrombosis in the leg or foot is a silent but dangerous condition. The key signs—unilateral swelling, persistent pain, warmth, redness, and heaviness—should never be ignored. While many cases are asymptomatic, recognizing risk factors and acting fast can prevent pulmonary embolism and chronic disability. If you notice unexplained leg symptoms, especially with known risks, seek evaluation immediately. With prompt diagnosis and treatment, DVT is manageable—and often preventable.