If walking barefoot across a tile floor feels like stepping on pebbles or hard bone, you may be experiencing fat pad atrophy in the heel—a degenerative condition where the natural cushioning under your heel thins and loses elasticity. This fatty tissue, known as the heel fat pad, acts as your foot’s built-in shock absorber, protecting the calcaneus (heel bone) from daily impact. When it deteriorates, every step becomes a source of deep, aching discomfort.
Often misdiagnosed as plantar fasciitis, fat pad atrophy is actually the second leading cause of plantar heel pain. Yet, it receives far less attention despite its significant impact on mobility and quality of life. Unlike plantar fasciitis, which causes sharp pain with your first steps in the morning, fat pad atrophy pain builds throughout the day and centers directly under the heel. The good news? While the lost fat doesn’t regenerate, symptoms can be effectively managed—and further damage prevented—with early recognition and proper care. This guide will help you identify the key signs of fat pad atrophy, distinguish it from other heel conditions, and explore proven treatment options.
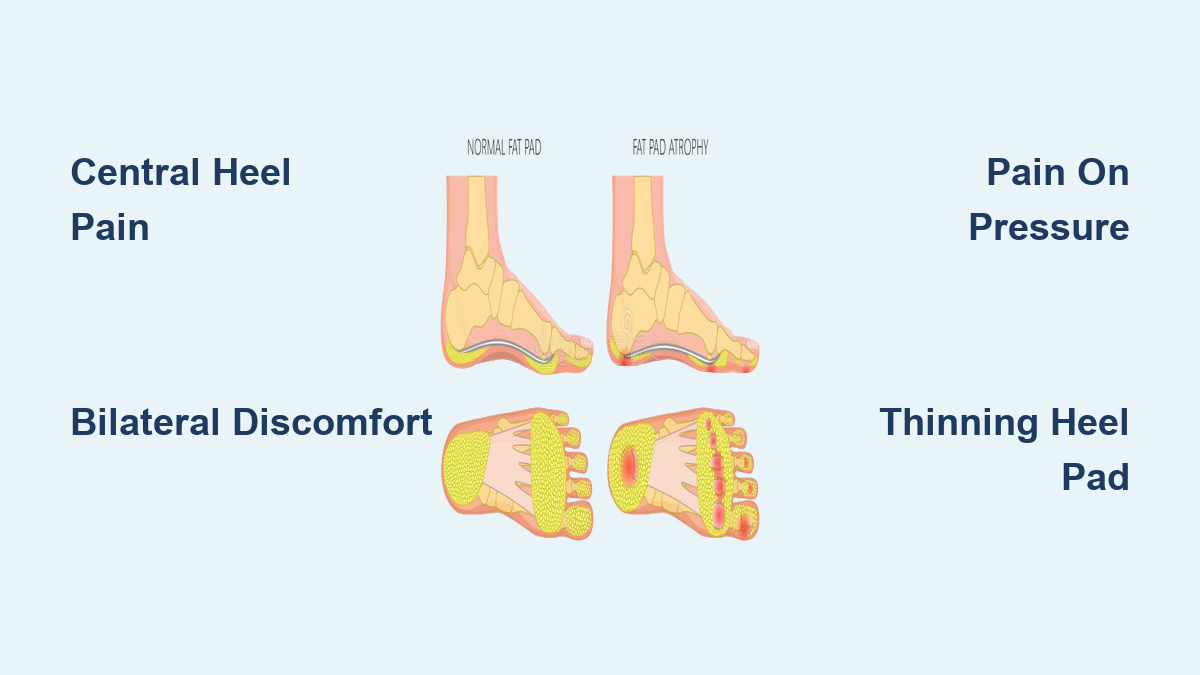
Central Heel Pain That Feels Like Walking on Bone
The most telling sign of fat pad atrophy is deep, bruise-like pain in the center of the heel. Patients often describe it as “walking on a rock,” “stepping on marble,” or feeling like their heel bone is hitting the floor with each step. This isn’t surface-level soreness—it’s a jarring, internal ache rooted in the loss of protective padding. Because the fat pad normally disperses force across the heel, its thinning means more pressure transfers directly to the bone, especially on hard surfaces like concrete, tile, or hardwood.
This pain typically flares during weight-bearing activities such as walking, standing, or running, and worsens as the day progresses. Many people find relief only when off their feet. This end-of-day pain pattern is a critical clue—unlike plantar fasciitis, which improves with movement, fat pad atrophy symptoms accumulate with use.
Pain When Pressing on the Center of the Heel
A simple self-test can help identify fat pad atrophy: press firmly on the middle of your heel. If this reproduces a deep, tender ache—especially compared to the sides or edges—it strongly suggests fat pad thinning. In contrast, plantar fasciitis causes pain more toward the inside front of the heel, near the arch. This difference in palpation location is one of the most reliable ways to differentiate the two conditions.
Bilateral Heel Pain: A Red Flag for Atrophy
Another key indicator is pain in both heels. While plantar fasciitis often affects one foot, fat pad atrophy tends to be bilateral, particularly when linked to aging, diabetes, or rapid weight loss. If you’re noticing similar discomfort in both feet, especially after long walks or standing at work, fat pad degeneration should be suspected.
High-impact activities—running, jumping, hiking—make symptoms worse due to increased load on the heel. Even routine tasks like grocery shopping or standing in the kitchen can become painful. Over time, this leads to reduced activity, which may contribute to broader physical decline.
Burning Sensation and Feeling of Walking on Rocks
As the condition progresses, some patients report a burning or raw feeling under the heel, especially after prolonged standing. This isn’t due to nerve damage like neuropathy but results from excessive pressure on sensitive tissues. Additionally, many describe a sensation of walking on an uneven or rocky surface, even on flat ground. This distorted perception occurs because the missing fat pad fails to evenly distribute pressure, creating localized “hot spots” of discomfort.
Visible and Tactile Signs of Heel Pad Thinning

Beyond pain, there are physical changes you can observe or feel that signal fat pad atrophy is underway.
Flattened or Sunken Appearance of the Heel
When standing, a healthy heel pad should appear plump and resilient, measuring 1 to 2 cm thick. In atrophy, the pad looks flattened or sunken, and the heel bone may appear more prominent. You might notice your foot looks “bony” underneath, especially when comparing weight-bearing and non-weight-bearing states. This thinning is gradual but becomes more obvious over time.
Stiffness and Loss of Elasticity
Press the center of your heel. A healthy fat pad will compress and spring back. In atrophy, the tissue feels stiff, hard, or unyielding—a sign of lost elasticity. Some patients, particularly those who’ve experienced rapid weight loss (e.g., from GLP-1 medications like Ozempic), also report saggy skin, visible veins, or a “deflated” look to the foot. These cosmetic changes often accompany functional decline.
Calluses, Corns, and Increased Ulcer Risk
With less cushioning, pressure shifts to bony areas, leading to calluses or corns on the heel or ball of the foot. These are the skin’s defense against friction and overload. In diabetic patients, this increased pressure raises the risk of foot ulcers—a serious complication. Any new skin thickening or breakdown under the heel should prompt evaluation, especially if you have diabetes or neuropathy.
What Causes Fat Pad Atrophy?
Fat pad atrophy develops from a mix of natural aging and external stressors that degrade the fat tissue over time.
Aging and Hormonal Changes
After age 40, the heel’s fat pad naturally begins to thin due to reduced collagen and elastin. Post-menopausal women are especially vulnerable, as declining estrogen levels accelerate tissue degeneration. This age-related wear is the most common cause.
Repetitive Impact and High-Load Activities
High-impact sports—running, basketball, gymnastics—subject the heel to forces up to 2.5 times body weight per step. Over time, this repetitive trauma damages fat cells, leading to microtears and atrophy. Even non-athletes are at risk if their job involves prolonged standing on hard floors.
Corticosteroid Injections and Trauma
Repeated corticosteroid injections near the heel—commonly used for plantar fasciitis—can cause fat necrosis, a known cause of iatrogenic (treatment-induced) atrophy. Similarly, past injuries like heel contusions or stress fractures can disrupt the fat pad’s structure.
Rapid Weight Loss and GLP-1 Medications
A growing concern: rapid weight loss from medications like Ozempic or Wegovy. These drugs can trigger sudden fat loss in the feet, outpacing the skin’s ability to contract. Patients report not only pain but also visibly sagging skin and loss of volume—a phenomenon dubbed “Ozempic feet.”
How It Differs from Plantar Fasciitis

Misdiagnosis is common because both conditions cause heel pain, but the timing, location, and response to activity differ.
Pain Location: Center vs. Medial Heel
Fat pad atrophy pain is central, directly under the heel bone. Plantar fasciitis pain is medial, closer to the arch. A simple finger test can reveal the difference: if pressing the middle of the heel hurts most, it’s likely fat pad atrophy.
Morning Pain vs. End-of-Day Pain
Plantar fasciitis causes first-step pain—sharp, stabbing discomfort upon waking. It usually improves with movement. Fat pad atrophy is often minimal in the morning and worsens with use, peaking by late afternoon.
Bilateral vs. Unilateral Involvement
Fat pad atrophy frequently affects both heels, especially in aging or systemic conditions. Plantar fasciitis is more often one-sided.
Confirming the Diagnosis
Accurate diagnosis starts with a clinical assessment and may include imaging.
Physical Exam and Medical History
Your provider will ask about pain patterns, activity level, and medical history—especially diabetes, steroid use, or recent weight loss. They’ll palpate the heel, assess pad thickness, and check for a heel-avoidance gait, where you walk on the ball of the foot to reduce impact.
Heel Pad Thickness Measurement
A normal heel pad is 1–2 cm thick when standing. Thinning below this range suggests atrophy. The provider may compare weight-bearing and non-weight-bearing thickness.
Imaging: Ultrasound and MRI
- Ultrasound: Quick and non-invasive; shows fat pad thinning and structure.
- MRI: Offers detailed soft tissue imaging; detects volume loss and microtears.
- X-ray: Rules out stress fractures or bone spurs but doesn’t show fat.
Treatment: From Support to Restoration
While the fat pad won’t regenerate, symptoms can be managed effectively.
Supportive Footwear and Cushioning
Wear shoes with thick, shock-absorbing soles, wide toe boxes, and good arch support. Avoid high heels, flip-flops, and worn-out shoes.
Heel Pads and Orthotics
- Gel or silicone heel cups: Provide 3–5 mm of cushioning.
- Custom orthotics: Molded to your foot, with padded top covers for extra protection.
Activity Modification and Weight Management
Reduce high-impact activities. Even a 5–10% weight loss can significantly reduce heel load. Combine with resistance training to preserve foot structure.
Ice and NSAIDs
Apply ice for 15–20 minutes after activity. Short-term NSAIDs (e.g., ibuprofen) can help manage pain.
Advanced Treatments for Severe Cases
Injectable Fillers
- Hyaluronic acid: 6–12 months of cushioning.
- Poly-L-lactic acid: Stimulates collagen; longer-lasting.
- Silicone: Risky due to migration and granulomas.
Autologous Fat Grafting: The Gold Standard
Fat is harvested from your abdomen or buttocks, processed, and injected into the heel. It restores volume and function.
- Recovery: No weight-bearing for 2 weeks; resume activity over 4–6 weeks.
- Success rate: Significant pain reduction up to 2 years post-procedure.
- Risks: Infection, fat resorption, asymmetry.
PRP and Regenerative Therapies
Platelet-rich plasma (PRP) may support healing, though evidence for fat regeneration is still emerging.
Prevention and Long-Term Foot Care
You can’t stop aging, but you can slow degeneration.
- Wear cushioned shoes daily—never go barefoot on hard floors.
- Avoid repeated steroid injections in the foot.
- Strengthen foot muscles with toe curls, marble pickups, and heel raises.
- Monitor skin changes, especially if diabetic.
Final Note: Fat pad atrophy in the heel is progressive but manageable. Key signs—central heel pain, tenderness to pressure, worsening with activity, and bilateral involvement—should prompt evaluation. Early intervention with proper footwear, orthotics, and lifestyle adjustments can prevent disability. For advanced cases, fat grafting offers a powerful solution. Don’t ignore heel pain—your mobility depends on it.