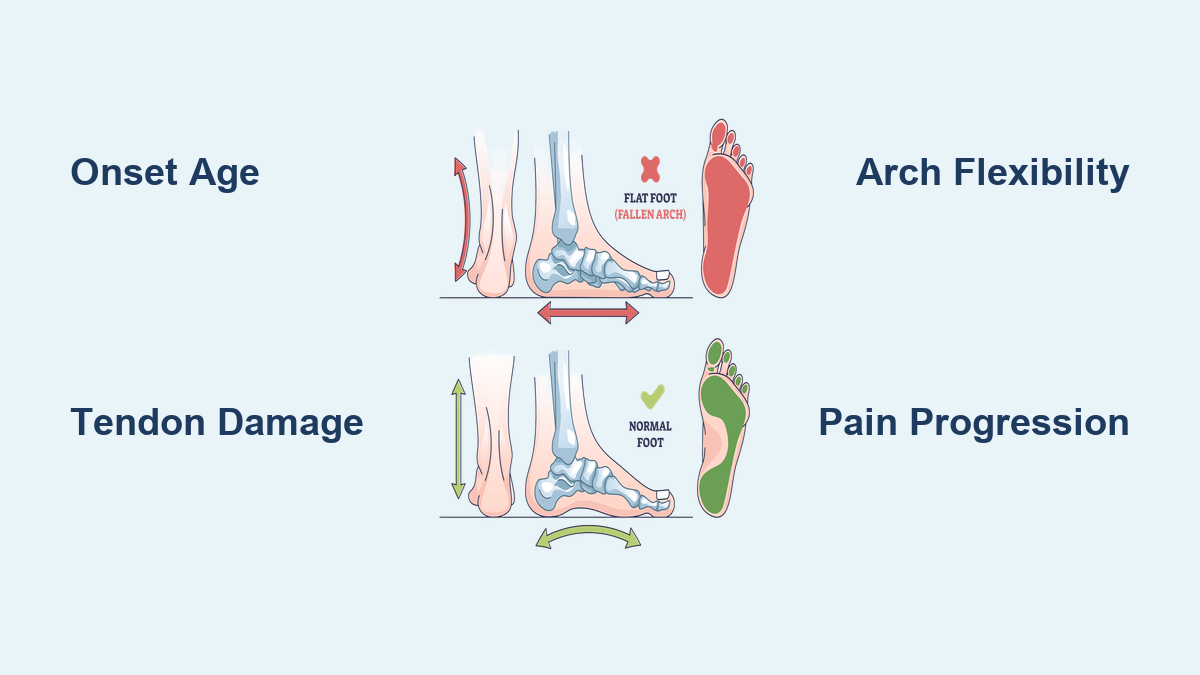
If one foot suddenly appears flatter than the other—especially if it’s accompanied by pain along the inner ankle—it may be a sign of a collapsed arch in one foot only, also known as unilateral adult-acquired flatfoot. Unlike lifelong flat feet, which typically affect both feet and are often painless, a one-sided arch collapse is progressive, painful, and usually linked to posterior tibial tendon dysfunction (PTTD)—a condition where the tendon that supports the arch becomes inflamed, weakened, or torn. This isn’t just a foot issue; it’s a biomechanical red flag that can lead to chronic pain in the ankle, knee, hip, and even the lower back if ignored. Recognizing early signs—like swelling, difficulty standing on tiptoes, or uneven shoe wear—can help you avoid surgery and preserve your mobility. This guide breaks down the key symptoms, causes, and what to do next if you suspect your arch has collapsed on one side.
Visible Flattening of the Arch in the Affected Foot

One of the most obvious signs of a unilateral arch collapse is a noticeable difference in foot shape. The affected foot will appear flat when standing, with the entire sole making more contact with the ground, while the other foot retains its normal arch.
Asymmetry Between Feet
Stand barefoot and compare your feet side by side. If one arch looks significantly lower—or has disappeared entirely—this asymmetry is a red flag. People with congenital flat feet usually have symmetry in both feet from childhood. But if you once had a normal arch that’s now visibly collapsed on one side, it’s likely an acquired condition, not a lifelong trait.
Positive Wet Footprint Test
A quick way to confirm arch collapse is the wet footprint test:
1. Wet the soles of both feet.
2. Step onto a dry surface like cardboard or a paper bag.
3. Examine the prints.
A normal arch leaves a narrow band of contact along the inner edge. A collapsed arch produces a full or nearly complete footprint. If only one foot shows this pattern, it confirms unilateral involvement and warrants medical evaluation.
Pain Along the Inner Ankle of the Affected Foot

Persistent discomfort along the inside of the ankle is often the first symptom—and it’s directly tied to posterior tibial tendon damage.
Location and Nature of Pain
The pain follows the path of the posterior tibial tendon, which runs behind the medial malleolus (the bony bump on the inner ankle). It may feel like a dull ache, sharp twinge, or throbbing sensation, especially after walking or standing for long periods. Touching the area may reveal tenderness or warmth, indicating inflammation.
Pain Worsens with Activity
This pain intensifies with weight-bearing activities like walking, hiking, or climbing stairs and eases with rest. Ignoring it can accelerate tendon degeneration and lead to permanent arch collapse.
Swelling Behind the Inner Ankle
Localized swelling on one side of the ankle is a key sign of tendon sheath inflammation.
Focused Swelling, Not Generalized
Unlike systemic swelling from conditions like arthritis or fluid retention, this puffiness is specific to the inner ankle—right where the posterior tibial tendon passes. The area may feel warm, tender, or spongy to the touch, and swelling often increases after activity.
Unilateral Presentation Is a Clue
If only one ankle swells—especially alongside arch flattening and pain—it strongly suggests unilateral tendon injury, not a generalized medical issue.
Inability to Rise on Tiptoes on One Side
Standing on your toes requires a strong posterior tibial tendon. When it fails, this motion becomes difficult or impossible.
Failed Single-Leg Heel Raise Test
Try standing on one foot and lifting your heel off the ground. If you can’t do this on the affected side, or it causes sharp pain, the tendon is likely compromised. This test is a cornerstone of clinical diagnosis for PTTD.
Functional Weakness and Instability
Even if you can rise, you may notice wobbling, inability to repeat the motion, or pain after a few reps. This indicates early-stage tendon failure and a need for intervention.
Toes Pointing Outward on the Affected Foot
As the arch collapses, the foot’s alignment shifts—a deformity called forefoot abduction.
The “Too Many Toes” Sign
Have someone view your feet from behind while standing. On the affected side, more toes will be visible on the outer edge due to the heel tilting outward (heel valgus). This classic clinical sign confirms progressive flatfoot.
Progressive Toe Drift
Over time, the toes of the affected foot may consistently point away from the body’s midline, especially when walking. This alters foot mechanics and increases strain on the ankle and knee.
Uneven Shoe Wear on One Side
Your shoes can reveal hidden foot problems. A collapsed arch changes how weight is distributed, leaving telltale wear marks.
Excessive Medial Sole Wear
Inspect the soles: the inner side (medial edge) of the heel and midfoot on the affected shoe will show significant wear. The unaffected foot may wear normally or on the outer edge.
Early Warning Before Severe Pain
Shoe wear asymmetry often appears before intense pain. Regularly checking your footwear can help catch arch collapse in its early, reversible stages.
Limping or Overpronation in One Foot
A unilateral arch collapse disrupts your natural gait, leading to noticeable imbalance.
Favoring the Unaffected Foot
You may shift weight to the good foot, creating a limp. This compensation can cause overuse injuries in the healthy foot, knee, or hip over time.
One-Sided Overpronation
The affected foot rolls inward excessively during walking (overpronation), destabilizing the lower limb. Watch your feet in a mirror while walking—you may notice one foot collapsing inward with each step.
Pain in the Knee, Hip, or Back
The body compensates for foot imbalance by adjusting posture, which can cause pain far from the foot.
Medial Knee Pain
The collapsed foot causes the tibia to rotate inward, increasing pressure on the inner knee. This mimics early medial compartment osteoarthritis.
Hip and Lower Back Strain
As one leg effectively “shortens” due to arch collapse, the pelvis may tilt, leading to hip pain or lower back strain. The discomfort is usually one-sided and worsens with prolonged standing.
Progressive Worsening of Symptoms
Unlike stable congenital flat feet, a unilateral collapse gets worse over time without treatment.
Stages of PTTD Progression
- Stage 1: Tendon inflammation—pain with normal arch.
- Stage 2: Flexible deformity—arch collapses but can be manually corrected.
- Stage 3: Rigid flatfoot—arthritis develops, arch cannot be restored.
- Stage 4: Ankle joint involvement—severe pain and instability.
Early detection (Stage 1–2) allows for non-surgical treatment. Delaying care increases the risk of needing surgery.
Causes of One-Sided Arch Collapse

Most cases stem from posterior tibial tendon dysfunction (PTTD), but several factors contribute.
Tendon Failure Due to Overuse or Injury
The posterior tibial tendon is the main dynamic support of the arch. When it’s overstretched, inflamed, or torn, the arch sinks. Trauma like an ankle sprain or repetitive strain from running can trigger unilateral failure.
Risk Factors
- Age over 40: Tendons weaken with age.
- Female gender: Hormonal influences may increase ligament laxity.
- Obesity: Extra weight strains the tendon.
- Diabetes or hypertension: Affect blood flow and tendon health.
- Previous ankle injury: Increases risk of asymmetric damage.
- Poor footwear: Shoes lacking arch support worsen stress.
How It Differs from Congenital Flat Feet
Not all flat feet are the same. Knowing the difference helps determine urgency.
Onset and Progression
- Unilateral collapsed arch: Develops in adulthood, progressive, painful.
- Congenital flat feet: Present from childhood, stable, often painless.
Flexibility and Function
- Collapsed arch: Initially flexible but worsens; tendon impaired.
- Congenital flat feet: Arch may reappear when non-weight-bearing; tendon intact.
Clinical Clue
If you used to have a normal arch that recently collapsed, it’s acquired—not congenital—and requires evaluation.
Diagnostic Tests by a Foot Specialist
If you suspect a collapsed arch, see a podiatrist or orthopaedic foot specialist.
Physical Examination
- Foot posture and gait observation.
- Tenderness along the posterior tibial tendon.
- Heel alignment and forefoot position.
- Single-leg heel raise test.
Imaging
- Weight-bearing X-rays: Show bone alignment and arthritis.
- MRI: Best for visualizing tendon tears or degeneration.
- Ultrasound: Detects tendon thickening or fluid.
- CT scan: Used for surgical planning.
Non-Surgical Treatment Options
Most early-stage cases respond well to conservative care.
Custom Orthotics and Supportive Footwear
- Prescription orthotics provide targeted arch support.
- Choose shoes with firm heel counter, medial support, and wide toe box (e.g., New Balance 928, Brooks Addiction Walker).
Physical Therapy Exercises
- Heel cord stretches: 4 sets of 30 seconds, twice daily.
- Single-leg calf raises: 3 sets of 15 reps.
- Towel scrunches: 3 sets of 10–15 reps.
- Arch lifts: Hold for 5 seconds, 10 reps.
- Balance training: Use a wobble board daily.
Activity Modification
Switch to swimming, cycling, or elliptical training. Avoid high-impact activities.
Medications and Bracing
- NSAIDs (e.g., ibuprofen) reduce pain and swelling.
- Ice therapy: 15–20 minutes after activity.
- Ankle braces or AFOs for moderate to severe cases.
When Surgery Is Needed
If conservative treatment fails after 6 months, or the foot becomes rigid, surgery may be necessary.
Common Procedures
- Tendon repair or transfer
- Osteotomy to realign bones
- Arthrodesis for arthritis
- Sinus tarsi implant to restore arch
Recovery
- Non-weight-bearing: 6–12 weeks
- Physical therapy follows
- Full recovery: 4–6 months
Prevention and Long-Term Care
Even after treatment, ongoing care is essential.
Daily Foot Strengthening
Walk barefoot on grass or sand. Do daily arch and ankle exercises.
Proper Footwear Habits
Avoid flip-flops or flat shoes without support. Replace worn shoes every 300–500 miles.
Weight Management
Maintain a healthy weight to reduce tendon load.
Monthly Foot Checks
Compare both feet for changes in arch height, swelling, or pain.
When to See a Specialist
Seek help if you notice:
– New flattening in one foot
– Persistent inner ankle pain
– Inability to rise on tiptoes
– Visible deformity
– No improvement after 4–6 weeks of home care
Early intervention can halt progression and avoid surgery.
Final Note: A collapsed arch in one foot is not just a foot problem—it’s a full-body biomechanical issue. Left untreated, it can lead to chronic pain in the ankle, knee, hip, and spine. But with early recognition and proper care, most cases can be managed effectively without surgery. Pay attention to asymmetry, pain, and function. Your feet support everything—don’t ignore the signs.