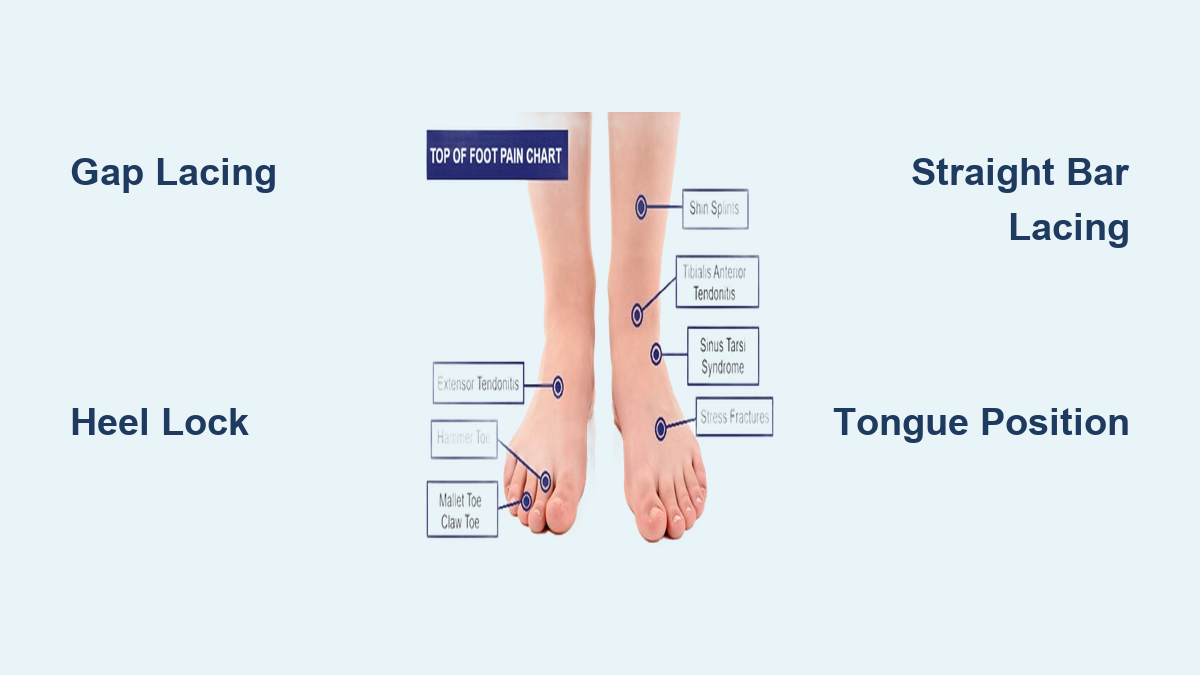
If you’re feeling a sharp ache, burning sensation, or dull throb along the outer edge of your foot—from the base of your little toe down toward your heel—you’re dealing with lateral foot pain, a surprisingly common issue that affects people of all ages and activity levels. Whether it flares up after a misstep, intensifies during a run, or appears without warning, this discomfort can make walking, standing, and even wearing shoes a challenge. The outer foot plays a vital role in balance and weight distribution, making it vulnerable to injury, overuse, and structural imbalances.
Understanding the root cause of your lateral foot pain is the first step toward effective treatment. It could be something as sudden as a fracture from rolling your ankle, or as gradual as tendonitis from years of overuse. This guide breaks down the most frequent causes, from traumatic injuries to chronic conditions, so you can recognize symptoms, know when to seek help, and take control of your recovery. With accurate diagnosis and targeted care, most cases of lateral foot pain can be resolved—often without surgery.
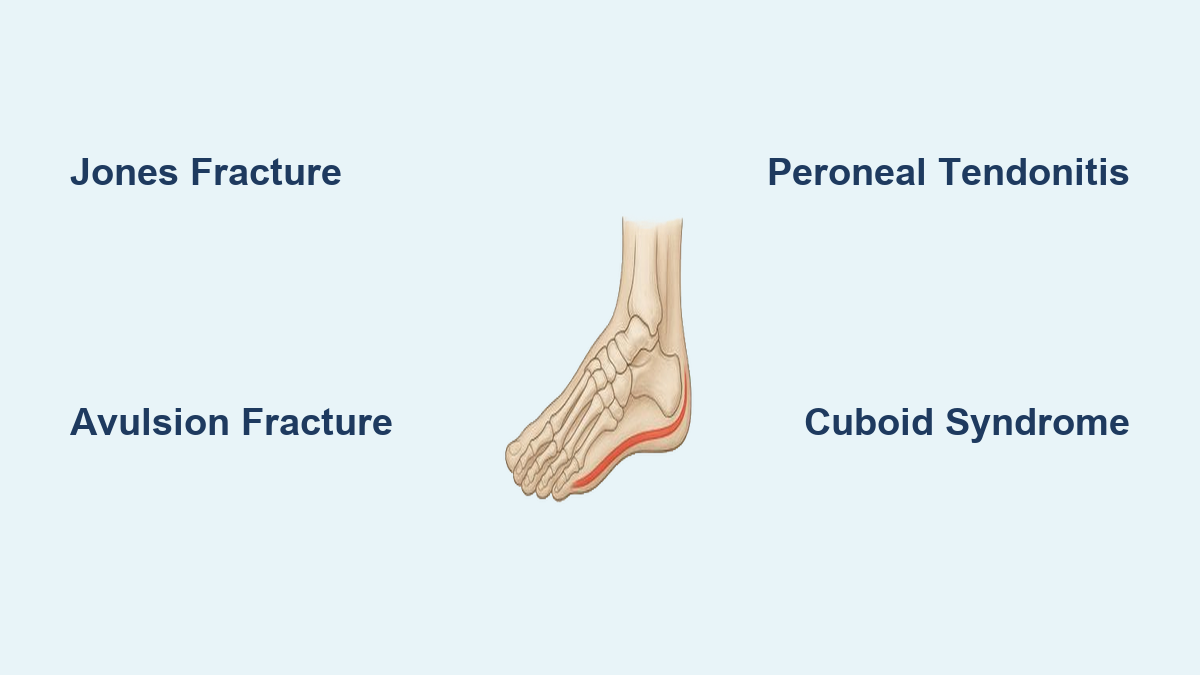
Jones Fracture: A High-Risk Break at the Base of the Fifth Metatarsal

One of the most serious causes of outer foot pain is a Jones fracture, which occurs in the upper portion of the fifth metatarsal—the long bone connected to your pinky toe. Unlike other fractures, this injury happens in a region with poor blood supply, significantly slowing healing and increasing the risk of nonunion (failure to heal).
This type of fracture often results from a sudden twist or inversion injury, such as stepping off a curb awkwardly or landing wrong during sports. Because the pain can resemble a sprain, it’s sometimes overlooked, leading to delayed treatment and complications.
Key symptoms include:
– Sharp, localized pain on the outer midfoot
– Swelling and tenderness at the base of the fifth metatarsal
– Increased pain when trying to walk or bear weight
Diagnosis starts with an X-ray, but early stress fractures may not appear for up to three weeks. If pain persists despite a normal initial X-ray, an MRI or bone scan is often needed to confirm the injury.
Treatment depends on severity:
– Non-surgical: Immobilization in a cast or walking boot with strict non-weight-bearing for 6–8 weeks. Bone stimulators may be used to encourage healing.
– Surgical: Most active individuals, athletes, or those with displacement are treated with intramedullary screw fixation to stabilize the bone and improve healing rates.
Returning to activity too soon can re-injure the area, so patience is critical. Full recovery typically takes 8–12 weeks.
Avulsion Fracture: Common After Rolling Your Ankle
An avulsion fracture happens when a small piece of bone is torn away by a ligament or tendon during an ankle roll. It’s one of the most common causes of immediate, sharp pain on the outside of the foot and is frequently mistaken for a simple sprain.
This injury usually occurs when the foot twists inward (inversion), pulling on the anterior talofibular ligament or peroneus brevis tendon, which then yanks a fragment from the base of the fifth metatarsal.
Signs to watch for:
– Sudden onset of pain and swelling
– Bruising on the outer foot
– Pain when pressing on the area or bearing weight
Unlike a Jones fracture, avulsion fractures occur in a region with better blood flow, so they typically heal well without surgery.
Recommended care:
– RICE protocol (rest, ice, compression, elevation)
– Use of a walking boot for support
– Gradual return to activity as symptoms improve
Most people recover within 4–6 weeks with conservative treatment.
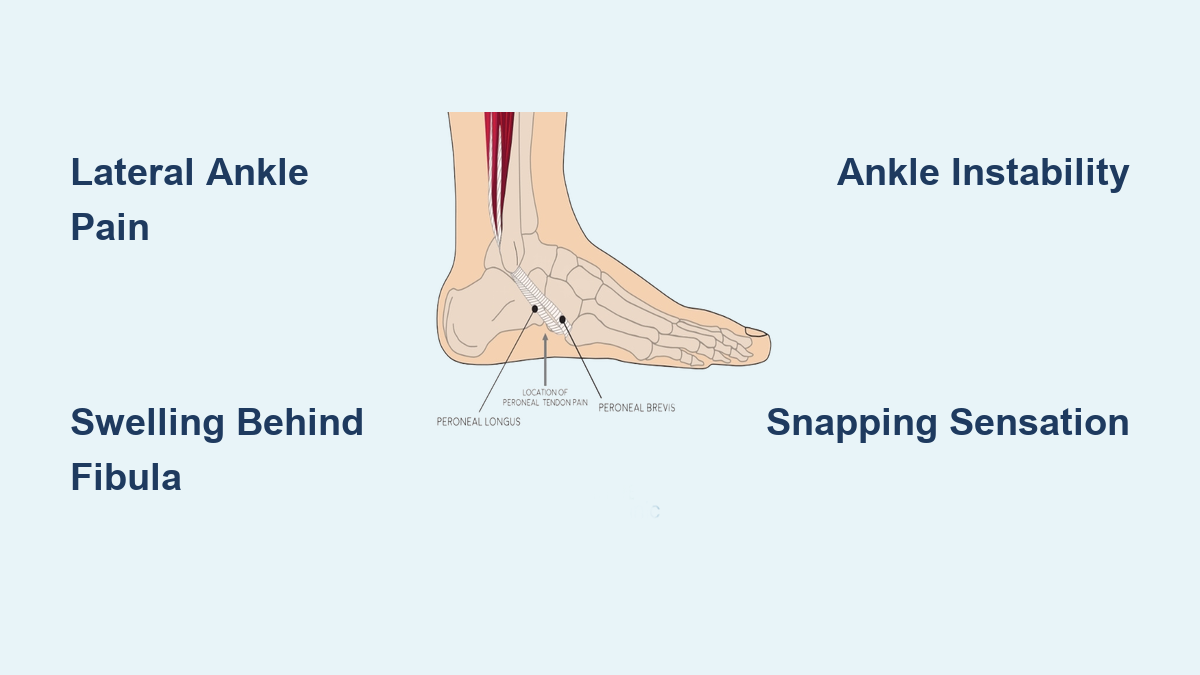
Peroneal Tendonitis: Overuse Pain Behind the Ankle
Inflammation or degeneration of the peroneal tendons—peroneus brevis and longus—is a frequent cause of outer ankle and foot pain, especially in runners, dancers, and individuals with high arches. These tendons run behind the lateral malleolus (the bony outer ankle) and help stabilize the foot during movement.
Overuse, previous ankle sprains, or poor foot mechanics can overload these tendons, leading to pain that worsens with activity.
Common symptoms:
– Pain behind or below the outer ankle, sometimes radiating toward the heel or arch
– Swelling or warmth along the tendon path
– A “snapping” or “popping” sensation may indicate subluxation (tendon slipping out of place)
Up to 60% of peroneal tendonitis cases are initially misdiagnosed as ankle sprains, delaying proper treatment.
Diagnosis involves:
– Physical exam: Tenderness with foot eversion or resisted movement
– Imaging: Ultrasound or MRI to detect inflammation, tears, or degeneration
Treatment options:
– Rest and activity modification
– Immobilization with a brace or boot
– NSAIDs to reduce pain and swelling
– Physical therapy focusing on strengthening, stretching, and balance training
In severe cases with tears or chronic instability, surgery may be needed to repair the tendon or deepen the fibular groove to prevent subluxation. Recovery ranges from 6 weeks (conservative) to 3–4 months (surgical).
Cuboid Syndrome: A Misaligned Bone in the Midfoot

Also known as a “dropped cuboid,” this condition involves subtle displacement of the cuboid bone in the lateral midfoot, often following an ankle sprain or repetitive strain. It’s common in dancers, runners, and people with high arches.
The injury typically occurs during a sudden twist with the foot pointed downward and inward (plantarflexion and inversion), causing the cuboid to shift out of place.
Symptoms include:
– Pain in the middle of the outer foot
– Increased discomfort when pushing off the foot or walking on uneven ground
– Tenderness directly over the cuboid
– Feeling like you’re walking on the side of your foot
X-rays may appear normal, so diagnosis relies on clinical tests like the midtarsal adduction test.
Treatment focuses on realignment:
– Manual reduction (cuboid whip): Performed by a podiatrist or physical therapist—often provides immediate relief
– Supportive care: Cuboid pad in shoe insert, taping, or custom orthotics
– Rehab: Stretching tight peroneal and calf muscles, strengthening intrinsic foot muscles
Most cases resolve within 2–4 weeks with proper treatment.
Ankle Sprain: The Most Common Cause of Lateral Foot Pain

Rolling your ankle inward (inversion) is the leading cause of outer foot and ankle pain. The lateral ligaments—especially the anterior talofibular ligament (ATFL)—stretch or tear, leading to swelling, bruising, and instability.
Symptoms:
– Sharp pain on the outer ankle
– Swelling, bruising, difficulty walking
– Feeling of “giving way,” especially with repeated sprains
Diagnosis:
– Physical exam checks for tenderness and joint laxity
– X-ray rules out fractures
– MRI if tendon or cartilage damage is suspected
Immediate treatment (RICE):
– Rest: Avoid weight-bearing
– Ice: 15–20 minutes every 2–3 hours
– Compression: Elastic bandage
– Elevation: Keep foot above heart level
Follow-up care includes bracing, taping, and physical therapy. Most sprains heal in 2–6 weeks, but untreated or repeated injuries can lead to chronic lateral ankle pain (CLAP).
Sinus Tarsi Syndrome: Deep Aching Pain After an Ankle Sprain
This condition causes deep, localized pain in the sinus tarsi—the small canal between the talus and heel bone—often after an ankle sprain or due to abnormal foot mechanics.
Symptoms:
– Pain between the ankle and heel on the outer side
– Worse with standing, walking on uneven ground, or turning the foot
– Feeling of instability or “giving way”
Diagnosis:
– Pain with palpation of the sinus tarsi
– Diagnostic injection: Pain relief after local anesthetic confirms the diagnosis
– MRI shows inflammation; CT rules out tarsal coalition
Treatment:
– Custom orthotics to stabilize foot motion
– Physical therapy
– NSAIDs or steroid injections
– Surgery (debridement) in persistent cases
Most improve within 4–8 weeks with conservative care.
Tailor’s Bunion: Bony Bump Aggravated by Tight Shoes
A tailor’s bunion (bunionette) is a bony prominence at the head of the fifth metatarsal, often caused by genetics or tight, narrow footwear.
Signs:
– Pain, redness, swelling at the bump
– Numbness if the nerve is compressed
– Discomfort when shoes rub the area
Non-surgical relief:
– Wear wide-toe-box shoes
– Use gel sleeves or padding
– Icing and NSAIDs
– Custom orthotics
Surgery: For severe cases—osteotomy or resection—followed by 4–6 weeks in a boot.
Arthritis: Chronic Joint Degeneration
Osteoarthritis or rheumatoid arthritis can affect joints on the outer foot, especially the subtalar or calcaneocuboid joints.
Symptoms:
– Chronic pain and stiffness, worse in the morning
– Swelling and reduced motion
– Pain with walking or standing
Diagnosis: X-ray shows joint space narrowing; MRI evaluates soft tissue.
Treatment: Orthotics, NSAIDs, steroid injections, or joint fusion in advanced cases.
Other Causes: Bursitis, Corns, and Tarsal Coalition
- Bursitis: Inflamed fluid sac under the fifth metatarsal head—treated with proper footwear and inserts.
- Corns and calluses: Thickened skin from shoe pressure—relieved with wider shoes and padding.
- Tarsal coalition: Congenital fusion of foot bones—diagnosed with CT/MRI; treated with orthotics or surgery.
Final Note: Lateral foot pain has many potential causes—from fractures and tendonitis to structural and degenerative issues. Accurate diagnosis is key. Start with rest, proper footwear, and self-care. If pain lasts more than 2–3 weeks, worsens, or limits daily life, see a foot specialist. Early treatment prevents chronic problems and gets you back on your feet faster.