Sharp pain in the heel bone can make even simple tasks like walking or standing unbearable. Whether it strikes with your first morning steps or flares up after a long day on your feet, this type of discomfort is more than just a minor nuisance—it’s often a warning sign from your body. While plantar fasciitis is the most common cause, accounting for the majority of cases, numerous other conditions can produce similar or even more intense pain. From stress fractures and nerve entrapments to systemic diseases like gout or rheumatoid arthritis, the root cause determines both the nature of the pain and the best path to relief.
Understanding the causes of sharp pain in the heel bone is essential for effective treatment. Misdiagnosing nerve-related pain as plantar fasciitis, for example, can delay proper care and prolong suffering. This guide explores the full spectrum of heel pain triggers, helping you identify potential culprits based on pain location, timing, and associated symptoms. You’ll learn how to distinguish between soft tissue injuries, bony abnormalities, nerve compression, and inflammatory conditions. We’ll also cover diagnostic steps, treatment options, and practical prevention strategies so you can take control of your foot health—before minor pain turns into chronic disability.
Common Soft Tissue Injuries

Most cases of sharp heel pain stem from overuse or strain of the foot’s connective tissues. These soft tissue conditions often develop gradually and are closely linked to biomechanics, activity levels, and footwear choices.
Plantar Fasciitis: The Leading Cause
Plantar fasciitis causes a sharp, stabbing pain under the heel, especially with the first few steps after waking. This occurs due to microtears and degeneration in the plantar fascia—a strong band of tissue that supports the arch and absorbs impact. Over time, repetitive stress leads to inflammation and pain, particularly at its attachment point on the bottom of the heel bone.
Key symptoms include:
– Pain that improves with movement but returns after prolonged standing
– Tenderness along the inner bottom of the heel
– Worsening pain when barefoot or on hard floors
Risk factors include age (40–60), obesity, flat feet, high arches, tight calf muscles, and jobs requiring long periods of standing. Runners and those who recently increased physical activity are also at higher risk.
Diagnosis is typically clinical, using the windlass test—where pain increases when the toes are pulled upward. Imaging like ultrasound (showing fascia thickness >4 mm) or MRI helps confirm the diagnosis or rule out other issues.
First-line treatments focus on reducing strain and promoting healing:
– Daily calf and plantar fascia stretches
– Custom or over-the-counter orthotics with arch support
– Night splints to maintain foot stretch overnight
– Ice therapy (15–20 minutes, 3–4 times daily)
– NSAIDs like ibuprofen for short-term pain relief
If pain persists beyond 6–12 weeks, advanced options include extracorporeal shockwave therapy (ESWT), MLS laser therapy, or corticosteroid injections—though these are used cautiously due to risks like fat pad atrophy. Surgery is rare, reserved for less than 5% of cases.
Heel Spurs: A Misunderstood Condition
Heel spurs are bony growths that form on the underside (plantar) or back (posterior) of the heel bone. They develop over time due to chronic tension in the plantar fascia or Achilles tendon, prompting calcium deposits. Crucially, most heel spurs are painless—only about 5% cause symptoms. When pain does occur, it’s usually due to inflammation in the surrounding soft tissues, not the spur itself.
Symptoms mimic plantar fasciitis: sharp heel pain with first steps, worsening after activity, and tenderness under or behind the heel. Diagnosis requires an X-ray, though MRI or ultrasound may be used to assess soft tissue damage.
Treatment focuses on the underlying cause—typically plantar fasciitis. This includes:
– Stretching and orthotics
– Supportive footwear
– Custom shoe inserts to redistribute pressure
Surgical removal is considered only if the spur causes mechanical issues and conservative care fails. Removing the spur without addressing biomechanics rarely resolves pain.
Achilles Tendinitis: Pain at the Back of the Heel
Achilles tendinitis involves inflammation or degeneration of the tendon connecting the calf muscles to the heel. Two types exist:
– Non-insertional: Affects the tendon’s midsection, common in active adults
– Insertional: Involves the tendon’s attachment to the heel bone, often with bone spurs
Symptoms include sharp or aching pain, stiffness, and swelling at the back of the heel—worsening with stairs, running, or jumping. The tendon may feel thickened or nodular.
Risk factors include sudden training increases, tight calves, wearing high heels, and age-related tendon wear.
Diagnosis involves physical exams like the Thompson test (to rule out rupture) and imaging (ultrasound or MRI) to assess tendon integrity.
Treatment includes:
– Heel drop exercises (Alfredson protocol)—proven to strengthen and heal the tendon
– Heel lifts in shoes to reduce strain
– Physical therapy with gait correction
– Avoiding corticosteroid injections near the tendon due to rupture risk
For persistent cases, platelet-rich plasma (PRP) injections, shockwave therapy, or surgical debridement may be needed.
Heel Bursitis: Inflammation of the Cushioning Sacs
Bursitis occurs when fluid-filled sacs (bursae) become inflamed. In the heel, two types matter:
Retrocalcaneal Bursitis
Located between the Achilles tendon and heel bone, often linked to Haglund’s deformity or insertional tendinitis.
Subcutaneous Calcaneal Bursitis
Found between the skin and heel bone, commonly caused by shoe pressure.
Symptoms include:
– Swelling, redness, and warmth at the back of the heel
– Pain when wearing closed shoes
– Tenderness and discomfort with movement
Treatment involves:
– Switching to soft-backed or open-heel shoes
– Ice and NSAIDs
– Heel pads to reduce friction
– Ultrasound-guided steroid injections for severe cases
– Surgery (bursa removal and bone reshaping) if chronic
Nerve-Related Causes of Heel Pain

Nerve compression syndromes often mimic soft tissue injuries but require different treatment approaches. Recognizing nerve-specific symptoms can prevent misdiagnosis.
Tarsal Tunnel Syndrome
This condition involves compression of the posterior tibial nerve behind the ankle. Symptoms include:
– Burning, shooting, or electric shock-like pain in the heel and sole
– Numbness or tingling in the arch, heel, or toes
– Pain that worsens with standing
– Positive Tinel’s sign: Tingling when tapping the nerve
Risk factors include flat feet, ankle swelling, diabetes, and space-occupying lesions.
Diagnosis uses nerve conduction studies (EMG) and MRI. Treatment includes:
– Custom orthotics
– Neuropathic pain medications (e.g., gabapentin)
– Steroid injections
– Surgical decompression if conservative care fails
Baxter’s Neuritis
Entrapment of the first branch of the lateral plantar nerve causes sharp, burning heel pain—often mistaken for plantar fasciitis. Clues include:
– Pain on the side of the heel rather than the center
– Radiating discomfort or night pain
– Minimal tenderness at the classic plantar fascia site
Diagnosis may require MRI (showing muscle edema) or a diagnostic nerve block. Treatment includes orthotics, physical therapy, and radiofrequency ablation—a highly effective outpatient procedure.
Bone and Joint Disorders
Some causes of heel pain originate in the bone or joint structures themselves.
Stress Fracture of the Heel
A stress fracture is a small crack in the calcaneus from repetitive impact. Symptoms include deep, aching pain that worsens with weight-bearing and may persist at night. Risk factors include sudden activity increases, osteoporosis, and vitamin D deficiency.
Diagnosis may require MRI or bone scan, as X-rays can be normal initially. Treatment involves:
– Non-weight-bearing or protected weight-bearing (boot, crutches)
– 6–8 weeks of rest
– Nutritional support (calcium, vitamin D)
Surgery is rare.
Haglund’s Deformity
Known as “pump bump,” this bony enlargement at the back of the heel irritates the Achilles tendon and bursa. Symptoms include a painful, swollen bump aggravated by rigid shoes. Treatment starts with soft footwear and heel pads; surgery reshapes the bone if needed.
Systemic and Inflammatory Conditions
Some full-body diseases manifest as heel pain.
Rheumatoid Arthritis (RA)
RA can cause bilateral heel pain with morning stiffness lasting over 30 minutes. Diagnosis involves blood tests (RF, anti-CCP) and imaging. Treatment includes DMARDs and biologics.
Gout in the Heel
Sudden, severe pain, redness, and swelling may indicate gout, caused by uric acid crystals. Diagnosis requires joint aspiration. Treatment includes colchicine, NSAIDs, and allopurinol for prevention.
Peripheral Neuropathy
Nerve damage from diabetes or toxins causes burning, stabbing pain, often worse at night. Treatment focuses on blood sugar control and neuropathic medications like pregabalin.
Traumatic and Degenerative Causes
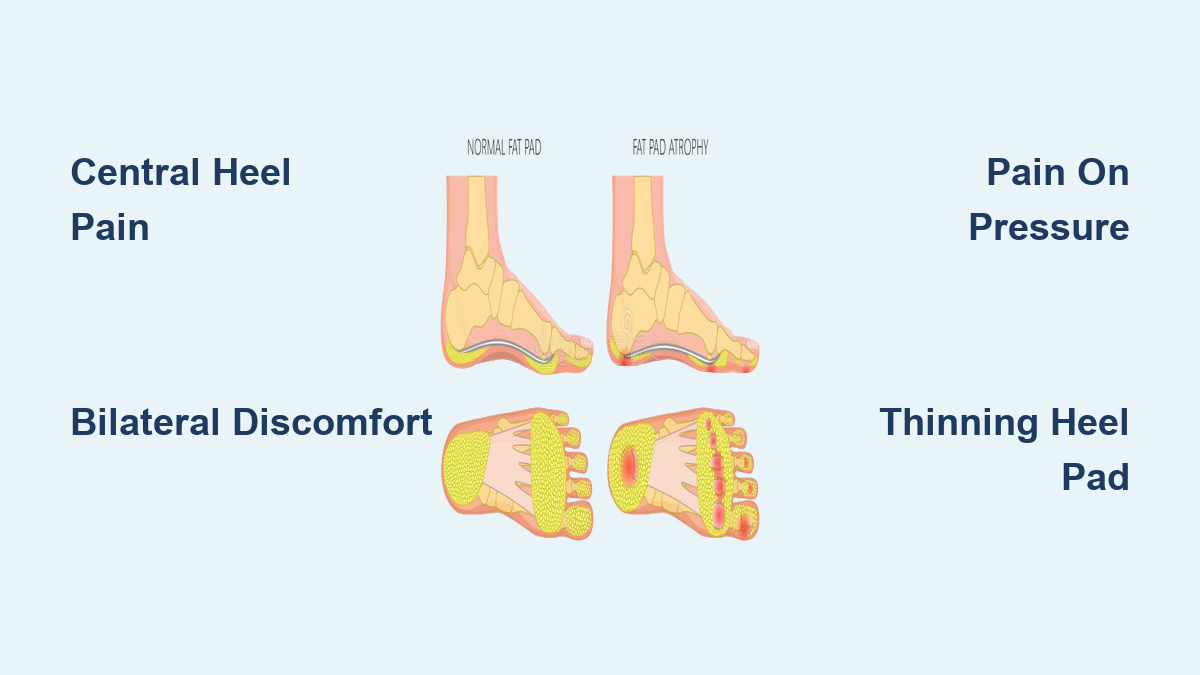
Heel Contusion and Fat Pad Atrophy
A bone bruise from trauma or thinning of the fat pad (common in older adults) leads to sharp, pebble-like pain under the heel. Treatment includes heel cups, cushioned shoes, and avoiding barefoot walking.
How Doctors Diagnose Heel Pain
Accurate diagnosis begins with:
– History: Onset, location, aggravating factors
– Physical exam: Palpation, gait analysis, Tinel’s sign, Thompson test
– Imaging:
– X-ray: For fractures, spurs
– Ultrasound: Dynamic tendon/fascia view
– MRI: Best for soft tissue, stress fractures, nerve issues
Treatment Comparison by Cause

| Condition | First-Line Treatment | Advanced Options |
|---|---|---|
| Plantar Fasciitis | Stretching, orthotics, night splints | ESWT, MLS Laser, PRP |
| Heel Spur | Treat underlying cause | Surgical excision |
| Achilles Tendinitis | Heel drops, rest, heel lifts | PRP, shockwave, surgery |
| Heel Bursitis | Shoe change, ice, NSAIDs | Steroid injection, surgery |
| Stress Fracture | Non-weight-bearing, rest | Nutrition, protected mobilization |
| Tarsal Tunnel | Orthotics, nerve meds | Surgical decompression |
| Baxter’s Neuritis | Conservative care | Radiofrequency ablation |
Prevent Sharp Heel Pain
Prevention is key:
– Maintain a healthy weight
– Wear supportive, cushioned shoes
– Stretch daily (calves, feet)
– Avoid prolonged standing
– Gradually increase activity
– Use orthotics if needed
– Never walk barefoot
– Choose low-impact exercises if prone to heel pain
When to See a Doctor
Seek help if:
– Pain lasts over 2–3 weeks
– You can’t walk normally
– There’s swelling, redness, or numbness
– Pain follows an injury
– You suspect gout or arthritis
A podiatrist or orthopedic specialist can provide accurate diagnosis and advanced care.
Final Note: Sharp pain in the heel bone is not something to ignore. While often treatable with conservative care, identifying the true cause—whether it’s plantar fasciitis, a nerve issue, or a systemic condition—is essential for lasting relief. Pay attention to your symptoms, act early, and protect your mobility. Your feet carry you every day—give them the care they deserve.