If you’re limping after your morning run or wincing with every step out of bed, the culprit might be a problem with your plantar fascia—the thick band of tissue that runs along the bottom of your foot, supporting the arch. But is it plantar fasciitis, a common overuse condition, or something more serious like a plantar fascia tear? While both cause heel and arch pain, they’re fundamentally different in cause, progression, and treatment. Misdiagnosing a tear as inflammation can lead to worsening injury, prolonged recovery, and even long-term foot deformity.
Understanding the signs of plantar fascia tear vs inflammation is crucial. One develops slowly and responds well to stretching and rest; the other strikes suddenly and often requires immobilization. This guide breaks down the key differences—onset, pain type, swelling, weight-bearing ability, and diagnostic findings—so you can recognize which condition you may have and seek the right care fast.
Plantar Fasciitis: Chronic Overuse and Tissue Degeneration
Despite its name, plantar fasciitis is less about acute inflammation and more about chronic degeneration of the plantar fascia due to repetitive stress. It’s the most common cause of heel pain, affecting millions each year, especially runners, people on their feet all day, and those with biomechanical imbalances.
Gradual Onset of Heel Pain Over Weeks or Months
Unlike a sudden injury, plantar fasciitis creeps in. You might notice mild discomfort that gradually worsens after long days at work, a new walking routine, or switching to unsupportive shoes. There’s no single moment of injury—just a slow buildup of pain that becomes hard to ignore.
Sharp Morning Pain That Eases with Movement
The telltale sign: stabbing pain with your first steps in the morning. This “post-static dyskinesia” happens because the fascia tightens overnight and gets painfully stretched when you stand. The pain usually improves within minutes or after light activity, but returns after prolonged standing or walking.
Tenderness at the Inner Heel, Not the Arch
Pressing on the bottom, inner part of the heel—where the plantar fascia attaches to the heel bone—reproduces the pain. It’s typically localized, not widespread, and rarely extends into the midfoot or toes.
No Bruising or Significant Swelling
While mild swelling may occur, bruising is uncommon in plantar fasciitis. The tissue is irritated and thickened, but structurally intact. If you see discoloration under your foot, think beyond simple inflammation.
Pain in Both Feet Is Possible
Because plantar fasciitis is often linked to systemic factors like obesity, flat feet, or tight calves, it frequently affects both feet, though one side may be worse. Bilateral heel pain is a strong clue pointing toward overuse rather than acute trauma.
Pro Tip: If your pain started slowly, is worst in the morning, and improves with walking, you’re likely dealing with plantar fasciitis—not a tear.
Plantar Fascia Tear: Acute Structural Damage
A plantar fascia tear means the fibrous band has partially or completely ruptured. This isn’t just sore tissue—it’s a structural failure that can happen during intense activity or even from minimal strain if the tissue is already weakened.
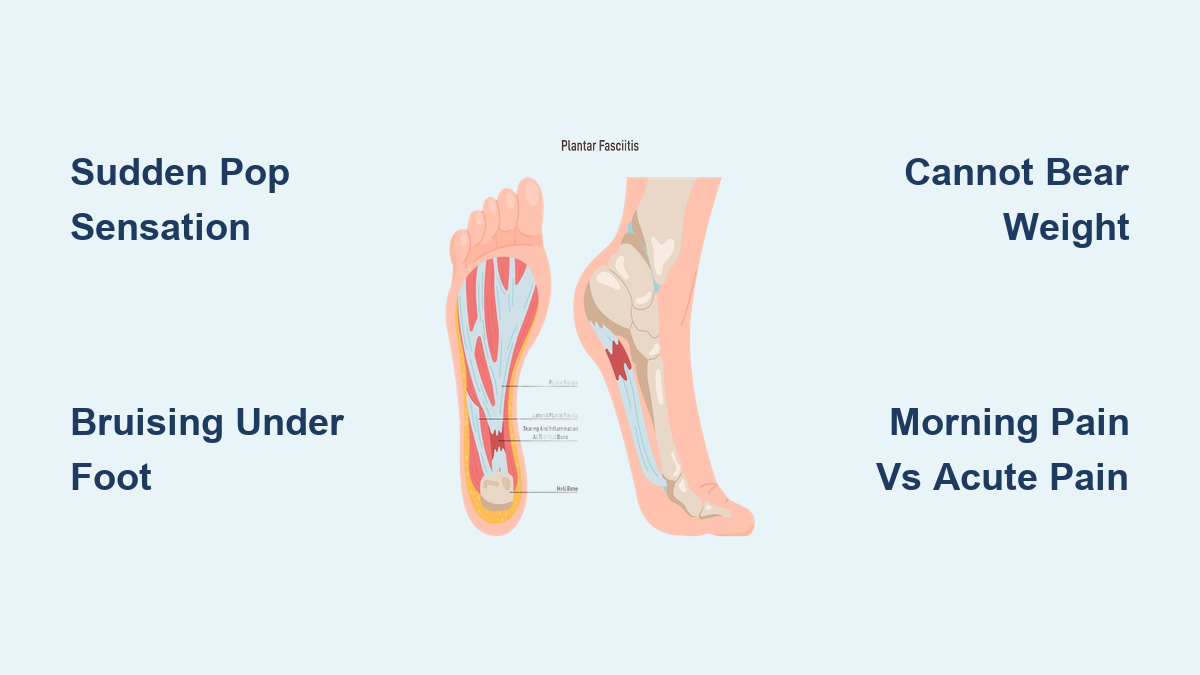
Sudden “Pop” or Tearing Sensation During Activity
Patients often describe feeling a snap, pop, or ripping sensation under the foot—especially during push-off while running or jumping. One second you’re moving fine; the next, you’re stopped in your tracks by sharp pain.
Patient report: “I felt a sudden tearing sensation under my heel, bringing me to an abrupt halt.”
This dramatic onset is a red flag. A “pop” under the foot should never be ignored.
Immediate Inability to Bear Weight
Most people can’t continue their activity after a tear. Many need crutches in the first few days. Even standing can be extremely painful, especially during the toe-off phase of walking, when the plantar fascia is under maximum tension.
Swelling and Bruising Along the Arch
Unlike plantar fasciitis, bruising and localized swelling are common with a tear. The discoloration—often under the arch or midfoot—results from internal bleeding at the rupture site. If you see purple or yellow bruising under your foot after sudden pain, suspect a tear.
Feeling Like You’re Walking on a Lump or Bunched-Up Sock
Due to tissue retraction or swelling, some patients report a lump-like sensation under the foot. This isn’t a growth—it’s the body’s response to the torn ends of the fascia pulling apart.
Possible Arch Collapse and Gait Changes
In a complete tear, the foot’s natural arch may flatten or drop, leading to instability. Over time, this alters your walking pattern, potentially causing pain in the ankle, knee, or hip.
Expert Note: A tear often occurs in someone with pre-existing plantar fasciitis. Chronic strain weakens the tissue, making rupture more likely—even during routine activity.
Key Differences in Symptoms and Onset

| Feature | Plantar Fasciitis | Plantar Fascia Tear |
|---|---|---|
| Onset | Gradual (weeks to months) | Sudden (seconds) |
| Pain Type | Dull ache, stiffness | Sharp, stabbing, “popping” |
| Morning Pain | Worse with first steps | Not specifically worse in AM |
| Bruising/Swelling | Rare | Common |
| Weight-Bearing | Painful but possible | Severely limited or impossible |
| Affected Foot | Often both | Usually one |
| Mechanism | Overuse, poor mechanics | Trauma, sudden force, or chronic strain |
Quick Check: Sudden pop + bruising + can’t walk = think tear. Morning pain + gradual onset + no bruising = likely fasciitis.
Why Misdiagnosis Happens and the Risks
Up to 50% of plantar fascia tears are initially misdiagnosed as plantar fasciitis because both cause heel and arch pain. Without a detailed injury history, clinicians may assume the more common condition.
Stretching a Tear Can Make It Worse
Treating a tear like fasciitis—by recommending stretching or aggressive loading—can pull the torn ends apart, delaying healing and increasing the risk of chronic pain or arch collapse. A tear needs protection; fasciitis needs mobilization.
Steroid Injections May Increase Rupture Risk
Corticosteroid injections, sometimes used for stubborn plantar fasciitis, can weaken collagen fibers in the fascia. While not all studies confirm this, many experts caution against repeated injections, especially in active individuals.
Clinical insight: “Most ruptures involve pre-existing plantar fasciitis. Chronic degeneration sets the stage for acute rupture.”
How Imaging Confirms the Diagnosis

When a tear is suspected, imaging is essential—clinical exams alone aren’t enough.
Ultrasound: Fast and Accurate for Soft Tissue
- Detects fascial thickening (>4 mm) in plantar fasciitis
- Shows gaps, discontinuity, or retraction in tears
- Allows real-time assessment during foot movement
Case example: After ruling out a fracture with X-ray, a diagnostic ultrasound clearly identified the tear.
MRI: Gold Standard for Severity
- Best for determining if the tear is partial or complete
- Reveals edema, tissue retraction, and healing response
- Rules out other causes like stress fractures or nerve entrapment
Expert quote: “Diagnosis is usually confirmed through an MRI scan, which helps determine the extent of the damage.”
X-Ray: Rules Out Bone Problems
- Not useful for soft tissue injuries
- Used to exclude heel spurs, stress fractures, or arthritis
Risk Factors You Can Control
Both conditions share triggers. Managing them reduces your risk.
- Obesity: Every pound adds 3–4x the force on your feet
- Tight calves (equinus): Increases fascial tension—stretch daily
- Flat feet or high arches: Use supportive orthotics
- Sudden activity spikes: Increase training by no more than 10% per week
- Poor footwear: Replace shoes every 300–500 miles
- Steroid injections: Limit to 1–2 per year, if used
Treatment: Why Approaches Differ
Plantar Fasciitis: Conservative Care Works
Most cases resolve in 6–12 months with:
– Stretching (calf and plantar fascia)
– Ice after activity
– Supportive shoes and orthotics
– Night splints and shockwave therapy if needed
Plantar Fascia Tear: Immobilization Is Key
- Stop weight-bearing immediately
- Use a walking boot (e.g., United Fracture Boot)
- Non-weightbearing for 2–3 weeks if complete tear
- Rigid arch supports to prevent collapse
- Gradual rehab with physical therapy
Study finding: In a 2004 athlete study, all returned to sport—average return time: 9 weeks.
Recovery Timeline Compared

| Phase | Plantar Fasciitis | Plantar Fascia Tear |
|---|---|---|
| Weeks 1–3 | Rest, ice, stretch | Non-weightbearing, boot |
| Weeks 3–6 | Light activity | Partial weight-bearing |
| Weeks 6–12 | Strengthening | Transition to shoes |
| Full Recovery | 6–18 months | 6–12 weeks (partial), up to 7 months (complete) |
| Return to Sport | After pain-free walking | Average 9 weeks |
Bottom line: A tear heals faster than chronic fasciitis—but only with proper initial care.
When to See a Doctor
Seek immediate evaluation if you experience:
– A popping sensation under your foot
– Sudden, severe pain in the arch or heel
– Bruising or swelling under the sole
– Inability to bear weight
For persistent heel pain lasting 2–3 weeks, see a podiatrist.
Final Note: The difference between plantar fascia tear vs inflammation isn’t just academic—it changes everything. One needs gentle loading and stretching; the other needs protection and rest. Know the signs. Get the right diagnosis. Heal faster.