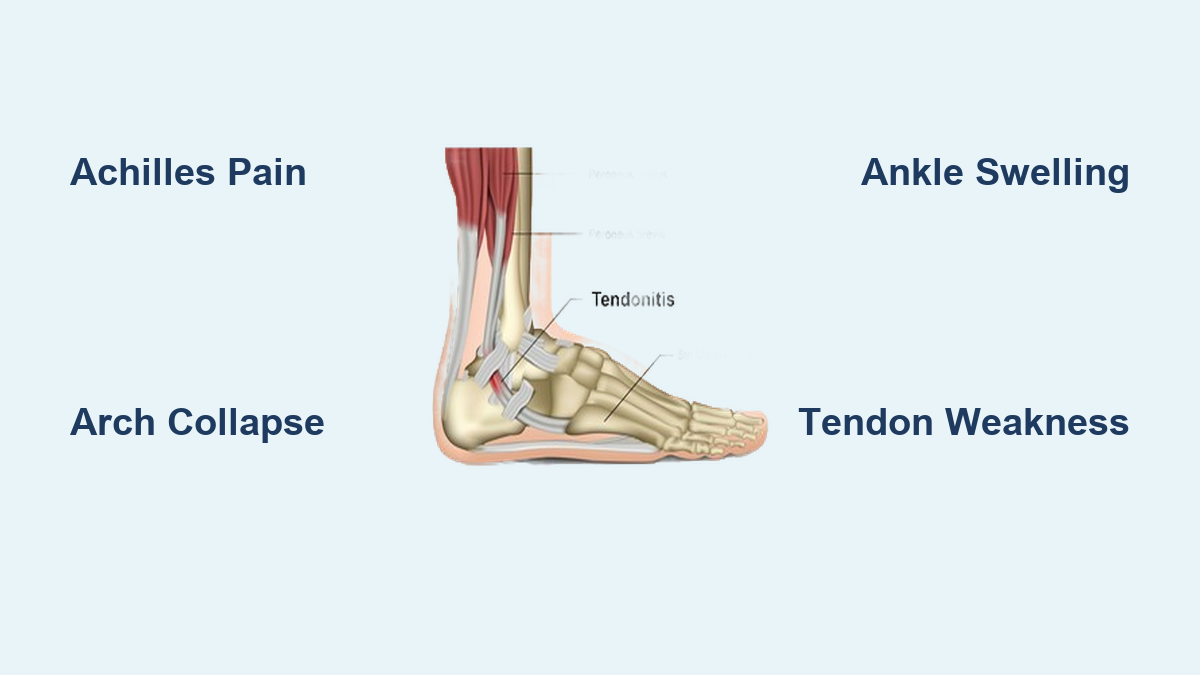
If you’ve ever limped after a long hike, struggled to rise onto your toes, or felt a persistent ache behind your ankle, you might be dealing with tendonitis in the foot and ankle. This condition occurs when tendons—strong, rope-like tissues connecting muscle to bone—become inflamed or irritated, typically due to overuse, repetitive strain, or acute injury. The foot and ankle rely on multiple tendons for movement and stability, and when one becomes damaged, even simple steps can turn painful.
Tendonitis isn’t just a temporary nuisance—it can progress from mild discomfort to chronic degeneration if ignored. While the term “tendonitis” suggests inflammation, modern medicine now recognizes that many long-standing cases are actually tendinopathy, a condition involving structural breakdown of the tendon without significant inflammation. Despite this distinction, both conditions share similar symptoms and treatment approaches. Early detection, accurate diagnosis, and proper management are crucial to prevent long-term complications like tendon rupture or permanent deformity. Whether you’re an athlete, a weekend walker, or someone on your feet all day, understanding foot and ankle tendonitis can help you take control of your mobility and recovery.
Commonly Affected Tendons in the Foot and Ankle

Multiple tendons support the foot and ankle, each vulnerable to strain depending on activity, biomechanics, and health. Identifying which tendon is involved helps guide treatment and recovery.
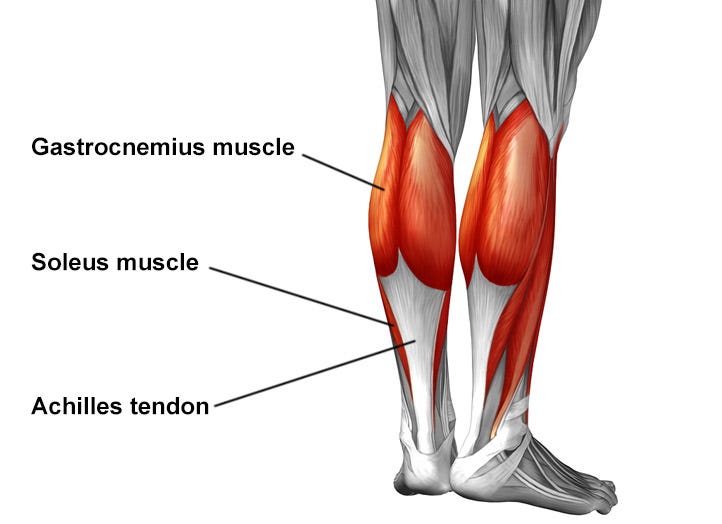
Achilles Tendon: The Body’s Powerhouse for Movement
The Achilles tendon, connecting your calf muscles to the heel bone, is the strongest tendon in the body. It enables walking, running, and jumping by facilitating plantar flexion—the motion of pointing your toes downward. However, its heavy workload makes it prone to injury. Achilles tendonitis typically causes pain and stiffness at the back of the heel or lower calf, especially in the morning or after activity. There are two main types:
– Insertional tendonitis affects the point where the tendon attaches to the heel bone and is often linked to bone spurs.
– Non-insertional tendonitis involves microtears and degeneration in the middle portion of the tendon, more common in younger, active individuals.
Ignoring symptoms can lead to partial tears or even a complete rupture, requiring surgical repair.
Posterior Tibial Tendon: The Arch’s Hidden Support
Running behind the inner ankle, the posterior tibial tendon plays a critical role in maintaining the foot’s arch. When inflamed, it leads to posterior tibial tendinitis, a leading cause of adult-acquired flatfoot. Pain develops along the inner ankle and arch, often worsening with walking or standing. As the tendon weakens, the foot may roll outward, collapsing the arch. A telltale sign—the “too many toes” sign—occurs when, viewed from behind, extra toes become visible due to foot abduction. Another diagnostic clue: difficulty performing a single-limb heel raise, where you can’t rise onto the toes of the affected foot.
Peroneal Tendons: Guardians of Lateral Stability
Located behind the outer ankle bone, the peroneal tendons (longus and brevis) stabilize the foot and prevent ankle sprains. Inflammation here, known as peroneal tendinitis, often mimics a lateral ankle sprain, making diagnosis tricky. Symptoms include pain on the outside of the ankle, swelling behind the fibula, and discomfort that worsens with resisted eversion (turning the foot outward). People with high arches or those who frequently run on uneven surfaces are at higher risk. If left untreated, the tendons may sublux (partially dislocate), requiring surgical correction.
Tibialis Anterior Tendon: Controlling the Front of the Foot
The tibialis anterior tendon runs down the front of the shin and helps lift the foot during walking—a motion called dorsiflexion. It also controls how the heel strikes the ground. When this tendon becomes inflamed, it causes anterior ankle pain, often worse at night or after activity. Pain increases with passive plantar flexion (pushing the foot downward). Overweight women and runners who rapidly increase mileage or train on hills are most susceptible. In severe cases, weakness can lead to foot drop, where the front of the foot drags during walking.
Flexor Tendons: Enabling Toe and Arch Function
Deep behind the inner ankle, the flexor hallucis longus and flexor digitorum longus tendons allow you to bend your toes and assist in arch support. Inflammation is rare but common in ballet dancers due to repetitive “en pointe” movements. Symptoms include pain along the arch and inner ankle, sometimes with a crunching sensation (crepitus) when moving the big toe. These injuries are often overlooked but can significantly impair push-off during gait.
Causes and Risk Factors Behind Tendonitis
Most cases of foot and ankle tendonitis stem from repetitive stress, but several contributing factors increase vulnerability.
Overuse and sudden increases in activity—like starting a new running program or hiking steep trails—overload tendons faster than they can repair. Acute injuries, such as ankle twists or direct impacts, can also damage tendons. Poor biomechanics, including flat feet or high arches, alter force distribution and strain specific tendons. Flat feet overwork the posterior tibial tendon, while high arches increase load on the peroneals.
External factors matter too: worn-out or unsupportive shoes, especially when running or standing for long periods, reduce shock absorption. Systemic conditions like diabetes, arthritis, and obesity impair healing and increase inflammation. Smoking reduces blood flow to tendons, slowing recovery. Even cold weather can make tendons stiffer and more prone to injury.
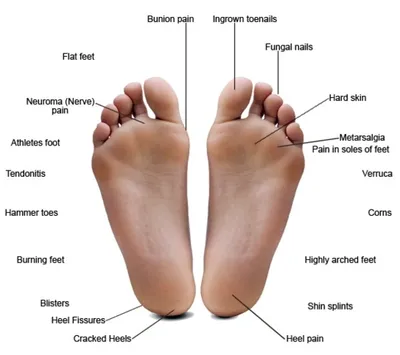
Recognizing the Warning Signs
Symptoms vary by tendon but commonly include localized pain, tenderness, swelling, and morning stiffness. Pain typically worsens with activity and improves with rest. You may notice weakness, such as struggling to rise on your toes or feeling unstable on uneven ground. A creaking or crunchy sensation (crepitus) during movement suggests tendon degeneration. In advanced cases, visible deformities like a collapsed arch or outward heel tilt signal chronic dysfunction.
How Doctors Diagnose Tendonitis

Accurate diagnosis starts with a detailed history—when symptoms began, what activities make them worse, and your footwear habits. A physical exam checks for swelling, tenderness, range of motion, and strength. Special tests include:
– Single-limb heel raise for posterior tibial function.
– Resisted eversion for peroneal involvement.
– Tibialis anterior stretch test to reproduce front-of-ankle pain.
Imaging confirms the diagnosis:
– X-rays rule out fractures or bone spurs.
– Ultrasound shows real-time tendon movement, thickening, or tears.
– MRI provides the most detailed view of soft tissue damage and is used when surgery is considered.
Conservative Treatment Options for Recovery
Most cases improve with non-surgical care, especially when treated early. The RICE protocol (Rest, Ice, Compression, Elevation) reduces inflammation and pain. NSAIDs like ibuprofen help manage discomfort, while topical gels offer targeted relief. Corticosteroid injections are used cautiously due to the risk of tendon weakening.
Supportive footwear with cushioning, arch support, and a firm heel counter is essential. Custom or over-the-counter orthotics correct biomechanical issues—arch supports for flat feet, lateral heel wedges for peroneal problems. Bracing or taping stabilizes the ankle during healing. In severe cases, a walking boot may be worn for 2–6 weeks to offload the tendon.
Physical Therapy: The Key to Long-Term Healing
Rehabilitation is critical. Eccentric strengthening exercises, like heel drops for Achilles tendonitis, rebuild tendon strength. Calf stretches relieve tension. Resistance band exercises improve posterior tibial function. Balance and proprioception training—such as single-leg stands or wobble board exercises—enhance stability and prevent reinjury.
Advanced and Surgical Treatments When Needed

If symptoms persist beyond 8–12 weeks, advanced therapies like platelet-rich plasma (PRP) injections or shockwave therapy (ESWT) may stimulate healing. Needle tenotomy removes damaged tissue, while nitroglycerin patches improve blood flow.
Surgery is reserved for failed conservative treatment or structural damage:
– Achilles tendon debridement removes degenerated tissue.
– Posterior tibial tendon transfer replaces a damaged tendon with a healthy one.
– Peroneal tendon repair fixes tears or deepens the fibular groove.
– Tibialis anterior debridement is effective when done within 5–25 months of symptom onset.
Preventing Tendonitis and Avoiding Recurrence
Prevention is key. Warm up with dynamic stretches like leg swings and ankle circles. Follow the 10% rule—don’t increase weekly activity by more than 10%. Wear proper footwear and replace running shoes every 300–500 miles. Use orthotics if you have flat feet or overpronation. Cross-train with low-impact activities like swimming. Most importantly, listen to your body—pain is a warning sign.
When to See a Doctor
Seek medical help if:
– Pain lasts more than 2–3 weeks despite rest.
– You can’t bear weight.
– Swelling or redness increases.
– You hear a pop or notice deformity.
Early care from a podiatrist or orthopedic specialist improves outcomes and prevents long-term disability.
Final Note: Tendonitis in the foot and ankle is treatable with prompt, informed care. Understanding the cause, recognizing symptoms, and taking action can restore mobility and prevent chronic issues. With the right approach, most people return to full activity—stronger and more resilient than before.