 Explained")
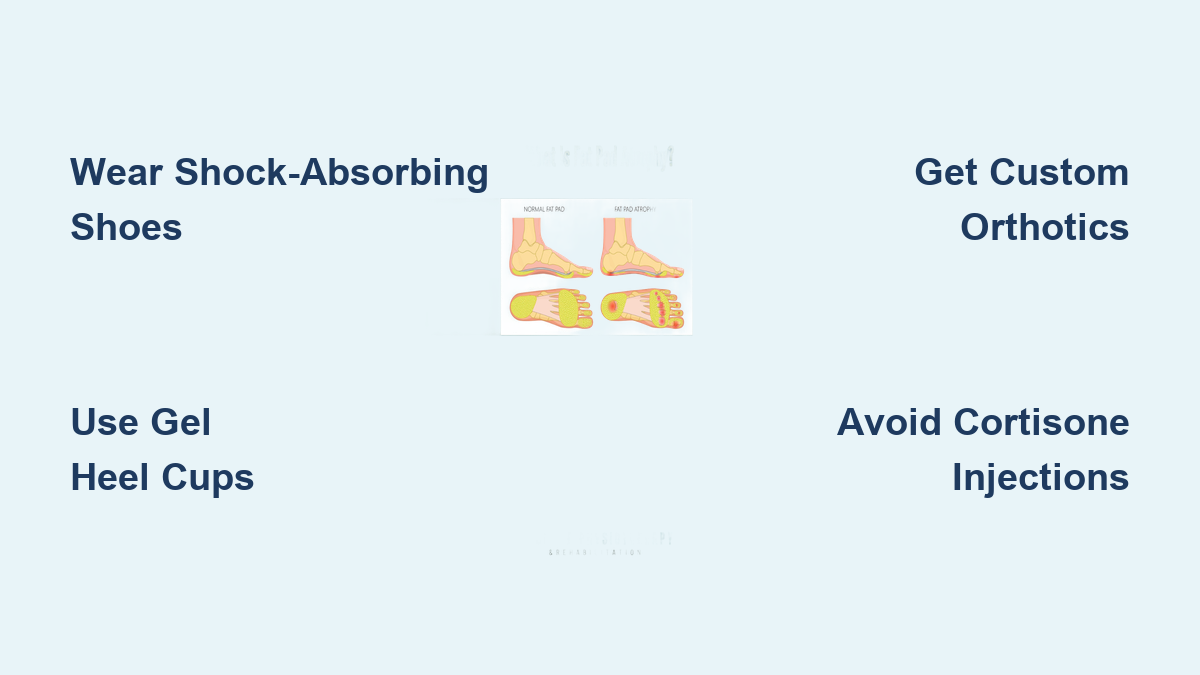
If you’ve been diagnosed with fat pad atrophy, every step may feel like walking on stone. This condition occurs when the natural fatty cushion beneath your heel thins or deteriorates, leaving the calcaneus (heel bone) exposed to direct pressure. Normally 1 to 2 centimeters thick, this specialized fat pad absorbs shock and protects the foot during weight-bearing activities. When it atrophies—often due to aging, trauma, obesity, or repeated corticosteroid injections—every movement becomes painful, especially on hard surfaces. The pain is deep, bruise-like, and worsens with activity, not in the morning like plantar fasciitis. But here’s the good news: you can effectively cushion the heel and reclaim your comfort.
With the right combination of footwear, orthotics, activity modification, and advanced treatments, you can reduce pain, protect your remaining fat pad, and prevent further damage. This guide provides a comprehensive, step-by-step approach to heel cushioning after fat pad atrophy, backed by clinical insights and real-world solutions. From choosing the best shoes to exploring regenerative injectables and surgical grafts, you’ll learn how to tailor your treatment to your severity level and lifestyle—so you can walk, stand, and live without fear of heel pain.
Choose Heel-Cushioning Footwear to Reduce Impact

Your shoes are the first line of defense against heel pain. Wearing the wrong footwear can accelerate fat pad degeneration, while supportive, shock-absorbing shoes can significantly reduce pressure on the calcaneus.
Avoid Barefoot Walking and Flat, Unsupportive Shoes
Walking barefoot—especially on tile, hardwood, or concrete—transmits 100% of your body weight directly to the heel. Without a protective layer, this causes microtrauma with every step. Similarly, flat shoes like flip-flops, ballet flats, or worn slippers offer zero cushioning and destabilize the foot. Even high heels are problematic: they shift weight forward but increase overall heel pressure during gait transitions. Avoid all unsupportive footwear and never go barefoot, even indoors.
Wear Shoes with Shock-Absorbing Soles and Heel Support
Look for athletic or medical-grade shoes that include:
– Thick midsoles made of EVA foam, gel, or air chambers
– Heel counters that stabilize the rearfoot and prevent excessive motion
– Rocker-bottom soles that reduce heel strike and promote a smooth roll-through gait
– Wide toe boxes to prevent compensatory pressure on the forefoot
Brands like Hoka, Brooks, New Balance, and Dansko offer models specifically engineered for heel pain and fat pad protection. These shoes are designed to mimic the natural shock absorption your body has lost.
Replace Worn-Out Shoes Every 300–500 Miles
Even high-quality shoes lose their cushioning over time. Check your footwear monthly for signs of wear: flattened heels, creased midsoles, or uneven tread. Replace athletic shoes every 300–500 miles, or sooner if you notice increased heel pain. A compressed midsole no longer absorbs impact—it just transmits force to your bones.
Use Heel Pads and Cushions for Immediate Relief

Adding internal padding helps compensate for lost fat volume and reduces peak pressure on the heel.
Insert Gel or Silicone Heel Cups
Gel and silicone heel cups fit inside your shoe and provide immediate cushioning. They:
– Absorb impact during heel strike
– Reduce vibration transmitted to the bone
– Center the heel to prevent slipping and friction
These are available over-the-counter and should be used in both shoes—even if only one heel is symptomatic—to maintain balanced gait mechanics.
Apply Self-Adhesive Pads for Targeted Protection
Foam, gel, or felt pads that stick to the foot or shoe lining offer extra protection in high-pressure zones. Use them:
– On areas of visible thinning
– When wearing dress shoes with limited space
– During long days on your feet
These are ideal for temporary relief or supplemental cushioning under orthotics.
Try Medical-Grade Foam Inserts Like Poron or Plastazote
Standard foam breaks down quickly under pressure. Poron and Plastazote are durable, compressible foams used in medical orthotics. They resist compaction, maintain shape, and can be trimmed to fit custom devices or shoes for long-term use.
Wear Custom Orthotics for Precision Heel Protection

While over-the-counter insoles offer some relief, custom orthotics are the gold standard for managing fat pad atrophy.
Get Medical-Grade Orthotics with Deep Heel Cups
Custom orthotics are made from a 3D scan or mold of your foot and designed to:
– Include deep heel cups that cradle and protect the remaining fat pad
– Add metatarsal pads to shift pressure away from the forefoot
– Correct biomechanical imbalances that increase heel loading
They distribute weight evenly across the foot, reducing focal stress on the heel and preventing compensatory injuries.
Avoid Generic Insoles That Lack Precision
Drugstore inserts often lack adequate heel depression or rearfoot control. They may feel soft initially but fail to offload the affected area effectively. For long-term management, custom devices are strongly recommended—especially if you’re active, overweight, or have high arches.
Modify Activities and Daily Habits to Reduce Heel Stress
Changing how you move and live can dramatically reduce strain on the heel.
Limit High-Impact Activities Like Running and Jumping
These generate forces up to 200% of your body weight per step—far too much for a compromised fat pad. Avoid prolonged standing, especially on hard floors.
Switch to Low-Impact Exercise
Stay active without damaging your heels:
– Swimming and water aerobics eliminate impact
– Cycling and elliptical training reduce heel loading
– Yoga and Pilates improve strength and flexibility safely
Use Anti-Fatigue Mats at Home and Work
If you stand for long periods (e.g., cooking or working at a counter), place cushioned floor mats on hard surfaces. These absorb shock and reduce cumulative stress on the heel.
Strengthen Feet and Retrain Your Gait for Better Support
Weak intrinsic foot muscles contribute to poor shock absorption. Strengthening them improves stability and reduces heel pressure.
Perform Daily Foot Muscle Exercises
Do these to support natural arches:
– Toe curls: Scrunch a towel with your toes (3 sets of 10)
– Marble pickups: Use toes to move marbles into a cup
– Short foot exercise: Contract the arch without curling toes
Perform twice daily to improve foot control.
Stretch Calf Muscles and Plantar Fascia
Tight calves increase heel strain. Stretch 2–3 times daily:
– Wall stretch: Lean into a wall with one leg back, heel down
– Step stretch: Hang heels off a stair for 30 seconds
Retrain Your Walking Pattern
A podiatrist or physical therapist can analyze your gait and teach you to:
– Land more midfoot rather than heel-first
– Shorten your stride to reduce impact
– Improve posture and alignment
Gait retraining can reduce peak heel pressure by up to 30%.
Moisturize and Protect Heel Skin to Prevent Discomfort
Thin, dry skin over the heel increases sensitivity.
Apply Emollients with Urea or Lactic Acid
Use creams containing 10–20% urea or lactic acid daily to keep skin supple and prevent cracking. Dry, callused skin reduces natural cushioning and adds to the sensation of hardness.
Avoid Skin Trauma
Wear seamless, cushioned socks even indoors. Avoid tight bands or rough fabrics that restrict circulation or cause abrasion.
Try Injectable Dermal Fillers for Volume Restoration
When conservative methods fail, injectable treatments restore cushioning.
Hyaluronic Acid (HA) Injections
HA fillers provide 6–18 months of cushioning. Benefits:
– Minimally invasive, in-office procedure
– Immediate effect
– Walk immediately after, but wear supportive shoes for 1–2 weeks
Poly-L-Lactic Acid (PLLA)
This collagen-stimulating filler requires 2–3 sessions and lasts up to 2 years. Ideal for long-term improvement.
Leneva (Allograft Adipose Tissue)
Leneva uses donated human fat to replace lost volume. It offers:
– Immediate cushioning and long-term regeneration
– All-natural, non-synthetic
– Lasts 2–5 years
– No risk of steroid-related atrophy
All injections use local anesthesia. Avoid high-impact activity for 4–6 weeks.
Consider Fat Grafting or Allograft Implantation
For severe cases, surgical-volume restoration offers lasting relief.
Autologous Fat Grafting
Fat is harvested from your body (e.g., abdomen), purified, and injected into the heel. Results last >5 years with a 98% success rate. Recovery: protected weight-bearing for 3 weeks.
Fat Pad Allografts
Donor-derived fat (e.g., 3cc) is implanted. No donor site surgery. Recovery: 6–8 weeks of protected weight-bearing. Lasts 5+ years.
Insurance coverage varies—seek pre-authorization.
Avoid Cortisone Injections at All Costs
Never use corticosteroid injections for fat pad atrophy. They can:
– Accelerate fat pad thinning
– Cause tissue atrophy
– Worsen long-term outcomes
If you’ve had heel injections and now have persistent pain, fat pad damage may be the cause.
Prevent Further Degeneration with Smart Habits
You can’t reverse atrophy, but you can slow it.
- Maintain a healthy weight—every extra pound adds 4x force to your heel
- Wear supportive shoes daily, even at home
- Avoid repetitive steroid injections
- Inspect and replace shoes monthly
See a Specialist If Pain Persists
Primary care often misdiagnoses fat pad atrophy as plantar fasciitis. See a podiatrist or foot and ankle specialist if:
– Pain worsens with activity
– You feel a “stone bruise” in the center of the heel
– Heel indentation is visible
– OTC remedies fail after 4–6 weeks
They can confirm diagnosis with weight-bearing ultrasound or MRI and offer advanced treatments.
Match Treatment to Your Severity Level
- Mild: Cushioned shoes, gel cups, activity changes, weight management
- Moderate: Custom orthotics, physical therapy, HA or Leneva injections
- Severe: Fat grafting, allografts, PRP, laser therapy
Final Tips for Long-Term Relief
- Layer your treatments for best results
- Act early to preserve remaining fat
- Custom solutions beat generic ones
- Avoid steroids
- Work with a specialist
With the right strategy, most patients achieve significant pain reduction and return to normal activities. Don’t accept chronic heel pain—protect your feet, cushion your steps, and reclaim your mobility.

