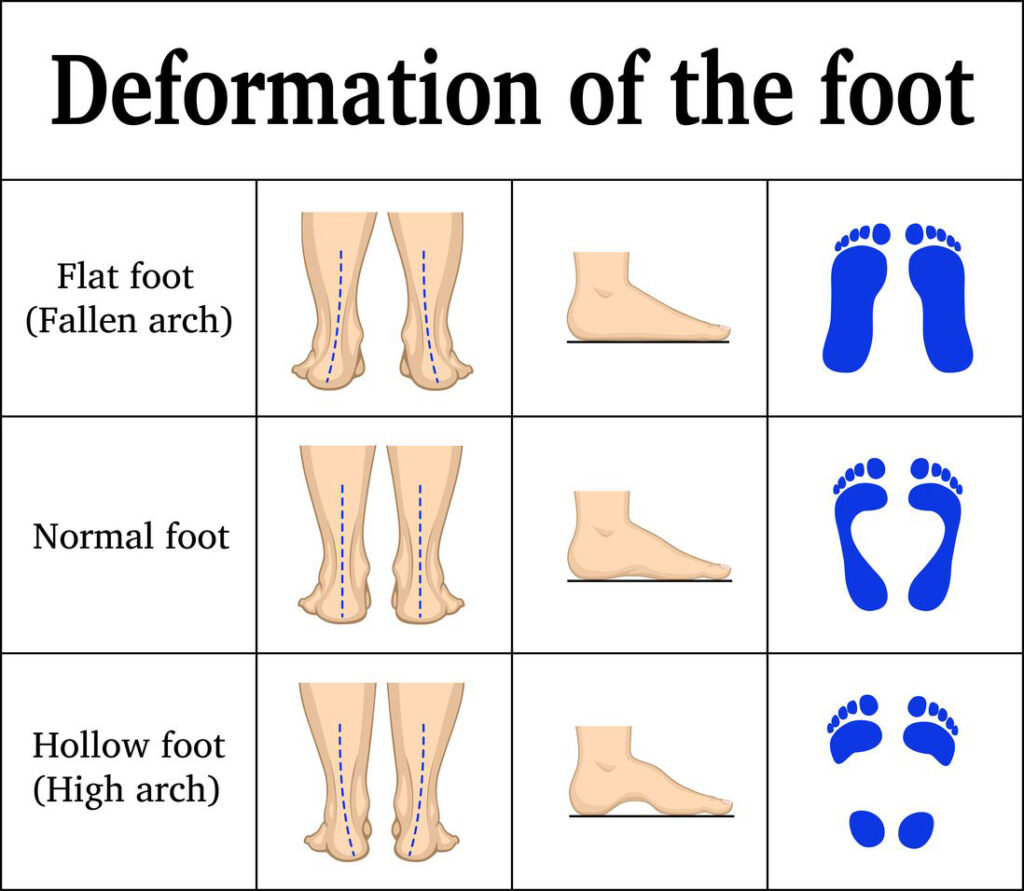
Flat feet in adults—medically known as pes planus or adult acquired flatfoot deformity (AAFD)—occur when the medial arch of the foot collapses, allowing the entire sole to press flat against the ground while standing. Unlike childhood flatfoot, which often resolves naturally, adult-onset cases are typically progressive, painful, and rooted in structural breakdown. The arch doesn’t just “fall” overnight; it deteriorates over time due to tendon failure, ligament damage, systemic disease, or mechanical overload.
The most common culprit is posterior tibial tendon dysfunction (PTTD), but aging, obesity, trauma, and chronic illnesses like diabetes and rheumatoid arthritis significantly accelerate the process. Left unchecked, flatfoot can lead to arthritis, chronic pain, and even spinal misalignment. Understanding the underlying causes is critical for early intervention. This guide breaks down the nine key factors behind adult flat feet—helping you identify risk, recognize symptoms, and take action before permanent damage occurs.
Posterior Tibial Tendon Dysfunction (PTTD): The Leading Cause

The posterior tibial tendon is the primary dynamic stabilizer of the foot’s arch. When this tendon weakens or tears, the arch begins to collapse—making PTTD the number one cause of adult flatfoot.
Why the Tendon Fails Over Time
This tendon runs from the calf, behind the inner ankle bone (medial malleolus), and attaches to the navicular and other midfoot bones. Its job is to lift and support the arch during walking and standing. However, with age, overuse, or injury, it can become inflamed (tendonitis), stretched, or even rupture.
Early signs include pain and swelling behind the inner ankle, especially after prolonged activity. You may feel your foot “giving way” or notice increasing fatigue in your legs. As the tendon deteriorates, the heel shifts outward (valgus tilt), and the foot rolls inward—classic overpronation.
Stages of Progressive Collapse
PTTD advances through four stages:
- Stage I: Inflammation with pain but no visible deformity. The arch remains intact.
- Stage II: Arch collapse begins. The foot becomes flexible and flat, and you cannot rise onto your toes on one foot.
- Stage III: Joints stiffen due to arthritis. The deformity becomes rigid.
- Stage IV: The ankle joint is affected, leading to instability and often requiring complex reconstruction.
A single-limb heel rise test during a clinical exam can detect Stage II dysfunction early. MRI or ultrasound confirms tendon damage and guides treatment.
Spring Ligament Failure: The Hidden Structural Weakness

While tendons provide dynamic support, the spring ligament (plantar calcaneonavicular ligament) acts as a passive arch sling—holding the talus bone in place and maintaining foot stability.
How Ligament Damage Triggers Collapse
Even with a healthy posterior tibial tendon, spring ligament rupture or elongation can cause flatfoot. This ligament supports the head of the talus; if it stretches or tears, the talus sinks downward, flattening the arch.
Injuries often occur due to trauma, chronic overpronation, or repetitive strain, but they’re frequently overlooked because symptoms mimic tendonitis. MRI is essential for accurate diagnosis, especially in younger adults with sudden flatfoot.
Who’s Most at Risk?
People with prior ankle sprains, connective tissue disorders, or obesity are more prone to spring ligament breakdown. The added mechanical load from excess weight accelerates wear, making early support critical.
Age-Related Degeneration of Foot Structures
After age 40, the foot’s tendons, ligaments, and joints naturally lose strength and elasticity. This cumulative wear-and-tear is a major contributor to adult flatfoot.
How Aging Undermines Arch Integrity
With time, the posterior tibial tendon thins, the spring ligament elongates, and cartilage in the midfoot joints wears down. These subtle changes reduce the foot’s ability to resist daily forces, especially during walking or standing.
Most cases emerge between ages 40 and 60, with women slightly more affected—possibly due to hormonal effects on connective tissue. While aging can’t be reversed, minimizing strain through supportive footwear and exercise can slow progression.
Obesity: The Weight That Breaks the Arch

Excess body weight is one of the most modifiable risk factors for adult flatfoot. Every extra pound multiplies stress on the arch during movement.
How BMI Impacts Tendon Health
During walking, the foot absorbs 3 to 5 times your body weight in force. In obese individuals, this constant overload speeds up degeneration of the posterior tibial tendon and spring ligament.
Studies show a direct correlation between high BMI and symptomatic flatfoot, particularly in middle-aged adults. Weight gain often precedes arch collapse and foot pain.
Can Weight Loss Reverse the Damage?
Losing 5–10% of body weight can significantly reduce foot pain, improve function, and even halt progression in early-stage flatfoot. Combined with orthotics and physical therapy, weight management is a cornerstone of non-surgical treatment.
Trauma: Sudden Injuries That Cause Flatfoot
A single event—like a fall, ankle sprain, or fracture—can instantly damage the arch’s supporting structures.
Common Injuries That Lead to Collapse
- Ankle fractures disrupting the medial column
- Severe sprains injuring the posterior tibial tendon or spring ligament
- Tendon ruptures from sudden twisting
- Lisfranc injuries compromising midfoot stability
These traumas may not cause immediate symptoms, but instability develops over time, leading to progressive deformity.
Delayed Onset After Injury
Some people develop flatfoot months or years after an untreated injury. A missed posterior tibial tendon tear, for example, may only become apparent when pain increases and the foot visibly flattens. If you’ve had a past foot or ankle injury and now notice new swelling or arch pain, get evaluated for AAFD.
Systemic Diseases That Undermine Foot Stability
Chronic medical conditions can weaken tendons, ligaments, and joints—making the foot more vulnerable to collapse.
Diabetes and Neuropathic Damage
Diabetes causes two major problems:
1. Peripheral neuropathy: Nerve damage reduces sensation, leading to unnoticed injuries and muscle imbalance.
2. Tendon degeneration: High blood sugar weakens collagen, increasing rupture risk.
In severe cases, Charcot arthropathy develops—where joints disintegrate painlessly, resulting in severe rocker-bottom deformity.
Rheumatoid Arthritis Destroys Midfoot Joints
RA attacks synovial tissue, causing inflammation and destruction of ligaments and joints. This leads to rigid, painful flatfoot with limited motion. Both feet are often affected, and surgical fusion may be needed to restore stability.
Hypertension and Vascular Damage
Though less direct, hypertension is linked to flatfoot in clinical studies. It may impair microcirculation to tendons, reducing oxygen supply and healing capacity. Often coexists with obesity and diabetes, compounding risk.
Connective Tissue Disorders
Conditions like Ehlers-Danlos or Marfan syndrome cause generalized ligament laxity. These individuals have naturally loose joints, making their feet less stable and more prone to early-onset flatfoot.
Childhood Flatfoot That Progresses Into Adulthood
Some adults who had flexible flatfoot as children experience worsening symptoms later in life due to decades of abnormal stress.
When the Arch Never Fully Developed
In childhood, flat feet are common and often resolve by age 10. But in some cases, the arch never forms. Initially painless, the foot undergoes repetitive strain—eventually leading to tendon fatigue and PTTD.
Symptoms typically emerge in mid-adulthood, especially after weight gain or increased activity.
Tight Achilles Tendon Alters Foot Mechanics
A stiff or short Achilles tendon limits ankle motion, forcing the foot to overpronate to compensate. This chronic inward rolling flattens the arch over time. The Silfverskiöld test can diagnose this issue, and treatment includes stretching or surgical lengthening.
Overuse From Repetitive Activities
Jobs or sports requiring prolonged standing, walking, or running place constant strain on the posterior tibial tendon.
High-Risk Occupations and Sports
- Military personnel
- Nurses and teachers
- Construction workers
- Runners and hikers
These groups face repetitive microtrauma that overwhelms the tendon’s ability to repair itself—especially with pre-existing risk factors.
Preventing Overuse Injury
Key strategies:
– Rotate high-impact activities with low-impact ones (e.g., swimming)
– Wear supportive, motion-control footwear
– Perform calf and foot strengthening exercises
– Use custom orthotics to reduce tendon strain
Early rest and intervention can prevent permanent deformity.
Poor Footwear Choices That Worsen Arch Support

Shoes lacking arch support, heel stability, or cushioning contribute to flatfoot progression.
How Bad Shoes Affect Foot Mechanics
Flip-flops, flat ballet shoes, or worn-out sneakers fail to control overpronation. Without medial support, the arch sinks further with each step, accelerating tendon fatigue.
A 2018 study found that populations wearing supportive shoes had lower rates of flat feet, though higher bunion prevalence—highlighting footwear’s complex biomechanical trade-offs.
Choosing the Right Shoes
Look for:
– Firm heel counter (resists squeezing)
– Arch support matching your foot shape
– Motion control features for overpronators
– Adequate cushioning for shock absorption
Brands like Brooks, ASICS, and Fitflop offer models designed for flat feet and stability.
Final Note: Adult flat feet are rarely due to a single cause—they result from a combination of structural, mechanical, and systemic factors. While posterior tibial tendon dysfunction is the most common trigger, obesity, aging, trauma, and diseases like diabetes or RA dramatically increase risk. Early detection through symptom awareness and clinical testing allows most cases to be managed without surgery. Custom orthotics, bracing, physical therapy, and lifestyle changes can halt progression and restore function. Left untreated, however, flatfoot leads to arthritis, chronic pain, and mobility loss. If you’re experiencing foot pain, swelling, or changes in foot shape, seek evaluation now—before the condition advances to irreversible stages.