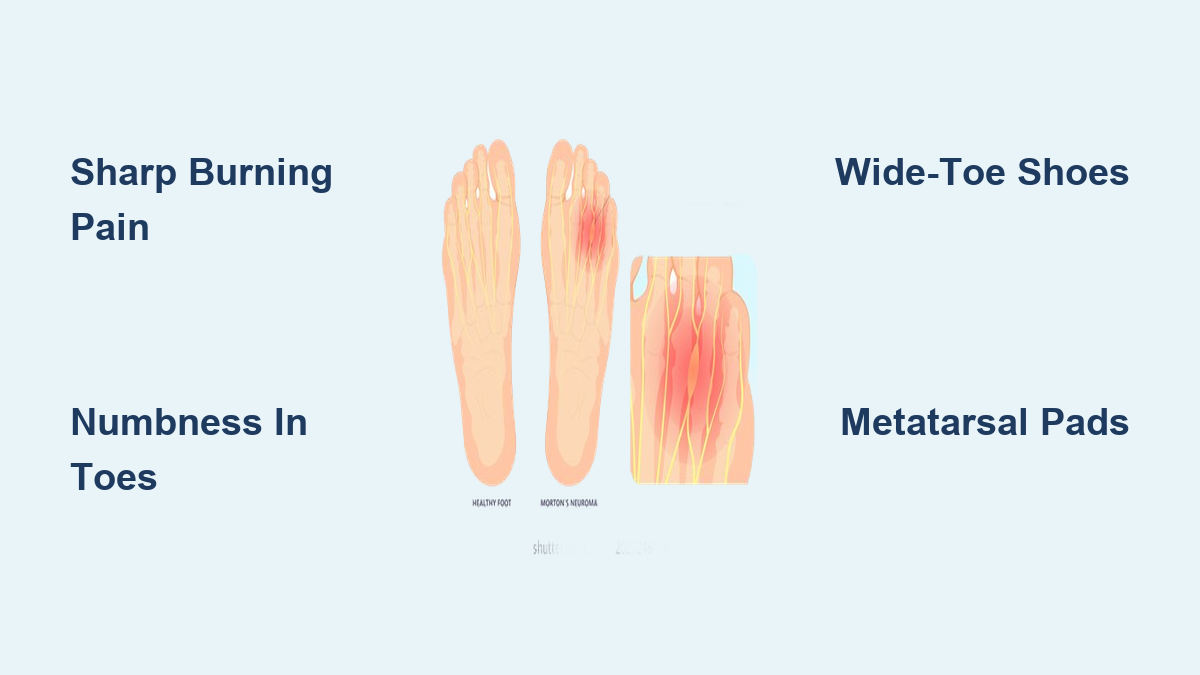
If you’ve ever felt like there’s a pebble in your shoe—except no matter how many times you stop to check, there’s nothing there—you may be experiencing Morton’s neuroma. This common foot condition causes sharp, burning pain, numbness, and tingling in the ball of the foot, typically between the third and fourth toes. Despite its name, Morton’s neuroma is not a tumor. It’s a benign thickening of nerve tissue caused by chronic compression or irritation of the interdigital nerve, usually between the metatarsal bones. Left untreated, it can lead to persistent pain and even permanent nerve damage.
Understanding what Morton’s neuroma is—and how it develops—is essential for effective treatment. Most cases occur in the third intermetatarsal space, where the nerve is naturally thicker due to the fusion of two nerve branches, making it more vulnerable to pressure. The condition disproportionately affects women, largely due to the frequent use of narrow or high-heeled shoes that squeeze the forefoot. It’s most commonly diagnosed in adults between 40 and 60 years old, though anyone with repetitive forefoot stress can develop it. The good news? Over 80% of patients improve with conservative care, including proper footwear, orthotics, and injections. This guide breaks down the anatomy, symptoms, causes, diagnosis, and treatment options so you can take control of your foot health.
Why the Third Web Space Is Vulnerable to Nerve Compression

The nerve most commonly affected in Morton’s neuroma runs between the third and fourth metatarsal heads—what’s known as the third intermetatarsal space. This location is especially prone to injury because the nerve here is formed by the fusion of two nerve fascicles, making it thicker and less flexible than other digital nerves. As a result, it has less room to glide when compressed between the metatarsal bones during walking or standing.
How the Intermetatarsal Ligament Contributes to Pain
Above this nerve lies the intermetatarsal ligament, a strong band of tissue connecting the metatarsal bones. During weight-bearing activities, this ligament can press down on the underlying nerve, especially if the metatarsals are squeezed together. This repeated pinching triggers inflammation, swelling, and eventually fibrosis (scar tissue formation) around the nerve. Over time, the nerve becomes thickened and hypersensitive, sending pain signals with even minor pressure—like walking in regular shoes.
Recognizing the Signs: Common Morton’s Neuroma Symptoms
Early detection improves outcomes, so it’s crucial to recognize the hallmark symptoms. These typically develop gradually and worsen with continued pressure on the forefoot.
Key Pain and Sensory Symptoms
- Sharp, burning, or stabbing pain under the ball of the foot
- Sensation of walking on a marble or small stone with no physical cause
- Feeling like a sock is bunched under the toes
- Numbness or tingling (paresthesia) in the third and fourth toes
- Electric-like shocks shooting into the toes during activity
These nerve-related sensations are distinct from joint or bone pain and usually affect only one foot, not both.
When Symptoms Get Worse (and Better)
Pain typically flares during:
– Walking or running, especially on hard surfaces
– Standing for long periods
– Wearing narrow or high-heeled shoes
Symptoms often improve when shoes are removed, the foot is rested, or the area is massaged. However, as the condition progresses, pain may persist even at rest. Some patients report a “clicking” sensation when pressure is applied—known as Mulder’s sign—which strongly suggests nerve entrapment.
What Causes Morton’s Neuroma? Key Risk Factors
Morton’s neuroma doesn’t appear overnight. It develops from long-term mechanical stress on the forefoot. While the exact cause varies, several major factors increase your risk.
Footwear That Triggers Nerve Irritation
- High heels (over 2 inches): Shift up to 75% more weight onto the ball of the foot
- Narrow or pointed toe boxes: Compress the metatarsals, squeezing the nerve
- Flat, unsupportive shoes: Transfer more impact to the forefoot
Women who regularly wear fashion footwear are at significantly higher risk.
High-Impact Activities and Jobs
- Runners, dancers, tennis players: Repetitive forefoot loading increases nerve stress
- Occupations requiring prolonged standing: Teachers, nurses, retail workers
- Hard flooring: Concrete or tile increases impact forces on the foot
Biomechanical Foot Issues
Structural imbalances alter pressure distribution:
– Flat feet (pes planus): Cause overpronation, stretching the forefoot
– High arches (pes cavus): Concentrate weight on the ball of the foot
– Bunions or hammertoes: Change toe alignment, increasing nerve compression
– Forefoot varus: The front of the foot tilts inward, pinching the nerve
Other Contributing Factors
- Obesity: Adds mechanical load to the forefoot
- Arthritis or joint inflammation: Swelling can compress nearby nerves
- Previous foot injuries: Altered gait patterns increase nerve stress
- Age-related fat pad loss: Natural cushioning under the foot diminishes with age
How Doctors Diagnose Morton’s Neuroma
Diagnosis begins with a detailed history and physical exam. Imaging may be used to confirm or rule out other conditions.
Clinical Evaluation: What to Expect
Your doctor will ask about:
– When symptoms started and how they’ve changed
– Your daily footwear and activity level
– What makes the pain better or worse
During the exam, they’ll:
– Look for calluses, swelling, or toe deformities
– Press between the metatarsal heads to check for tenderness
– Test sensation and strength in the toes
Diagnostic Tests That Confirm the Condition
Mulder’s Sign (Whisper Sign)
- The doctor squeezes the metatarsals together while pressing on the web space
- A positive test causes pain, tingling, or a palpable click
- Highly suggestive of Morton’s neuroma
Squeeze Test
- The sides of the forefoot are compressed
- Reproduction of interdigital pain supports nerve entrapment
Imaging to Confirm or Rule Out Other Issues
Ultrasound
- First-line imaging for dynamic assessment
- Can detect nerve thickening (usually >4 mm)
- Helps differentiate neuroma from bursitis
MRI
- Best for soft tissue detail
- Shows nerve enlargement and surrounding inflammation
- Used if surgery is being considered
X-ray
- Does not show the neuroma
- Rules out stress fractures, arthritis, or bone spurs
Conditions That Mimic Morton’s Neuroma
Not all forefoot pain is a neuroma. Accurate diagnosis is critical.
Metatarsalgia
- Generalized forefoot pain under the metatarsal heads
- Lacks nerve-specific symptoms like numbness or tingling
Metatarsal Stress Fracture
- Pain is often on top of the foot (dorsal)
- Confirmed by MRI or bone scan
Lumbar Radiculopathy
- Caused by a herniated disc
- Includes low back pain and leg symptoms
Tarsal Tunnel Syndrome
- Causes burning or tingling along the inner sole of the foot
Synovitis or Capsulitis
- Inflammation of the joint lining, often in the second toe
- Pain is joint-centered, not nerve-based
Bursitis
- Inflammation of fluid-filled sacs
- May appear as a compressible mass on ultrasound
Conservative Treatment: How to Relieve Symptoms Without Surgery

Over 80% of patients improve with non-surgical care, though it may take 3 to 6 months.
Fix Your Footwear First
- Switch to wide-toe-box shoes with low heels (<2 inches)
- Choose soft, cushioned soles
- Avoid pointed, tight, or high-heeled shoes
Use Orthotics and Metatarsal Pads
- Custom or OTC orthotics redistribute pressure
- Metatarsal pads lift and separate the metatarsal heads
- Arch supports correct flat or high arches
Medications for Pain and Swelling
- NSAIDs (ibuprofen, naproxen) reduce inflammation
- Acetaminophen for pain if NSAIDs aren’t suitable
- Topical capsaicin may help desensitize nerves
Physical Therapy and Exercises
- Calf and plantar fascia stretches reduce strain
- Towel curls, marble pickups strengthen foot muscles
- Gait training corrects abnormal walking patterns
- Shockwave therapy may help chronic cases
Injection Therapies
Corticosteroid Injections
- Lidocaine + steroid reduces inflammation
- Provides relief for weeks to months
- Limited to 2–3 injections to prevent tissue damage
Alcohol Sclerosing Injections
- 4% alcohol solution damages nerve tissue to reduce pain
- Given in 3–7 sessions, 1–3 weeks apart
- Success rate: 70–80% in resistant cases
Botox Injections
- May relax muscles and reduce nerve compression
- Not standard care; limited evidence
Surgical Options for Persistent Morton’s Neuroma
Surgery is considered when conservative treatment fails after 6 months.
Neurectomy: Removing the Affected Nerve
- Most common surgery
- The nerve is cut and removed
- Success rate: 80–95%
- Drawback: Permanent numbness between the toes
- Recovery: 2–4 weeks in a surgical shoe, full recovery in 2–3 months
Nerve Decompression (Neurolysis)
- The intermetatarsal ligament is cut to relieve pressure
- Preserves nerve function—no numbness
- Success rate: 80–90%
- Preferred for active patients
Post-Surgery Recovery Tips
- Limited weight-bearing for 1–2 weeks
- Wear a protective shoe
- Gradual return to regular footwear over 4–6 weeks
- Physical therapy may help restore strength and gait
Preventing Morton’s Neuroma: Smart Foot Habits
You can reduce your risk significantly.
Wear Foot-Friendly Shoes
- Low heels (<2 inches)
- Wide toe box with room for toes
- Cushioned soles for shock absorption
Use Orthotics If Needed
- Custom inserts for flat or high arches
- Metatarsal pads to offload pressure
- Replace insoles every 6–12 months
Strengthen and Stretch Your Feet
- Daily toe exercises: Towel scrunches, marble pickups
- Calf stretches: Prevent tightness that shifts weight forward
- Roll a ball under the foot to massage the arch
Maintain a Healthy Weight
- Every extra pound increases forefoot pressure
- Weight loss reduces load and inflammation
When to See a Doctor
Don’t wait if pain is affecting your life.
Red Flags
- Pain lasts more than two weeks despite home care
- You can’t walk comfortably or wear normal shoes
- Numbness or tingling is spreading or worsening
- Symptoms don’t improve after changing footwear
Who to Consult
- Podiatrist: Foot and ankle specialist
- Orthopedic surgeon: If surgery is needed
- Physical therapist: For gait and muscle training
Early diagnosis prevents chronic pain and nerve damage.
Final Note: Morton’s neuroma is a treatable condition that mimics a tumor but is actually a reactive nerve thickening from chronic compression. It most often affects the third web space and causes burning pain, numbness, and a sensation of walking on a stone. Diagnosis is clinical, supported by Mulder’s sign, ultrasound, or MRI. Over 80% of patients improve with conservative care—especially proper footwear, orthotics, and injections. Surgery is highly effective for stubborn cases. Prevention focuses on foot mechanics and smart shoe choices. If your forefoot pain persists, seek professional help early to avoid long-term complications.